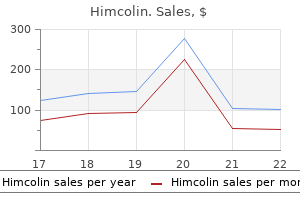
Himcolin 30 gm line
Tumors which are localized within the myocardium usually lead to impotence foods discount 30 gm himcolin overnight delivery impaired myocardial operate either through substantial replacement of the myocardium by tumor or due to extension right into a cardiac cavity impotence used in a sentence 30 gm himcolin discount with mastercard. Intramural location could lead to erectile dysfunction treatment vancouver himcolin 30 gm buy discount on-line all kinds of rhythm disturbances, including atrial fibrillation and ventricular fibrillation. Tumors may much less generally come up in the best atrium and much much less typically the ventricles. Although historic debate about this has occurred, myxomas may also originate from any cardiac valve. Myxomas are normally gentle and friable with a particular gelatinous look and consistency. Some myxomas could additionally be firm, and occasionally gross calcifications could also be observed, even to the extent that the bulk of the tumor consists of a calcified mass. The surgeon, aware of the risk of recurrence after excision, will usually remove the tumor along with its web site of origin. Thus, in atrial myxoma, the surgical specimen virtually actually will include a through-andthrough section of the atrial septum or of the atrial wall. Histopathology Microscopically, the tumors are dominated by a myxomatous matrix and a dispersed cellular element. The cytoplasm is usually homogeneous, is typically finely vacuolated, and is often barely eosinophilic. Mitoses are nearly absent and, when present in additional than an occasional cell, should increase suspicion that the tumor could additionally be a sarcoma, somewhat than myxoma. The massive polyhedral myxoma cells are sometimes referred to additionally as "lepidic cells" (from the Greek lepis meaning "scale" and based on a somewhat fanciful resemblance to the scales on butterfly wings). At the ultrastructural level the cytoplasm of a "typical" myxoma cell is characterised by scant organelles. Variable numbers are seen of mitochondria, elements of clean and rough endoplasmic reticulum, and cytoplasmic filaments. The majority are thick (10 nm) nonbranching filaments, typically arranged in parallel bundles coursing in numerous directions. These clusters of myxoma cells are often related to an intensive halo of myxoid extracellular matrix, virtually optically empty, which contrasts with the encircling and barely extra condensed matrix that stains palely eosinophilic. Other cell varieties that might be current embrace elongated, spindle-shaped cells that resemble fibroblasts, myofibroblasts, or clean muscle cells. Macrophages are an virtually universal discovering in myxomas, often diffusely dispersed throughout the myxoid stroma, although generally condensed towards the bottom and at websites of hemorrhage. These cellular aggregates occur predominantly within the base of the tumor and can additionally be discovered in the adjacent myocardium. It incorporates variably outstanding connective tissue fibers having traits of reticulin, collagen, and elastin. Fibrous tissue is most pronounced within the stalk of the tumor, a web site often dominated by the presence of huge, thick-walled (and sometimes dysplastic) arteries. The "tumor blush" often noticed at coronary angiography has its anatomic substrate on this vascular tuft. It is essential to emphasize that, like the cellular components, the stroma may show intensive variability from one part of the tumor to the other. Distinct fibrous areas and foci of liquefaction of the myxoid stroma, leading to cyst-like areas, could additionally be seen. Although barely extra pronounced in surgical specimens than in post-mortem instances,14 these foci are most probably the consequence of trauma resulting from the mobile nature of the intracavitary tumor. Occasionally these may be so outstanding that the tumor itself is overshadowed and never easily recognized. In approximately 5% of cardiac myxomas gland-like constructions occur, lined by cells which will vary from flat to cuboidal or columnar. Thymic epithelial rests may also be seen in myxomas (as properly as in the myocardium) and may often turn into so proliferative as to warrant the designation "thymoma". The observation that myxomas may contain epithelial, as properly as mesenchymal, components has advised to some that they need to be categorized as hamartomas. Valvular myxomas reportedly have fewer mobile clusters, fewer syncytial tumor large cells, and more rare perivascular cuffing of tumor cells than myxomas occurring elsewhere. Recurrence of a cardiac myxoma after surgical excision is a relatively uncommon but undisputed phenomenon. Most instances of malignant myxomas doubtless represent cases of misdiagnosis14,40,forty one or the inclusion of false metastases based mostly on "invasiveness" of embolized myxoma fragments, causing ischemic infarction and subsequent infiltration of the arterial wall and/or extracardiac parenchyma. Nevertheless, the potential of malignant transformation of cardiac myxomas stays a matter of concern with three potential instances having been reported, one with glandular components. The myxoma cells are reactive with antibodies to calretinin (75%) and vimentin (50%). Calretinin may be notably helpful in differentiating myxoma from different entities. Differential Diagnosis Cardiac myxomas can probably be confused with any number of different neoplasms that arise in or involve the heart (Table 2-5). Myxomas can be differentiated from organizing thrombi by the presence of attribute myxoma cells and matrix. Thrombi on the floor and foci of organizing intratumoral hemorrhage can occasionally make this distinction difficult, and calretinin stains could additionally be useful within the distinction, because the cells of organizing thrombi fail to react with this antibody. Papillary fibroelastomas have extra advanced papillary structure, lack the myxoid stroma, and nonetheless have characteristic avascular elastic fiber cores. The main histopathologic features to distinguish between a benign cardiac myxoma and the myxoid variant of so-called undifferentiated high-grade pleomorphic sarcoma (myxofibrosarcoma)47,forty eight are foci of hypercellularity with pleomorphism, mitotic figures, necrosis, and intensive vascularity in myxofibrosarcoma, features which are strikingly absent in cardiac myxomas. Cytogenetic analysis of cardiac myxomas, up to now, has proven a big selection of clonal and nonclonal abnormalities. As it stands now, cytogenetic evaluation is of little or no value in the differential analysis of cardiac myxomas, although these studies could eventually contribute to understanding their molecular pathogenesis. Rhabdomyoma Clinical Features this is certainly one of the extra frequent main tumors of the guts and by far the most typical in infants and youngsters. A smaller proportion happen sporadically or in association with congenital heart disease. Because of its improvement in utero, the medical presentation could differ from that of another cardiac tumors. In some instances, the tumor could have led to stillbirth or perinatal demise,fifty six,fifty seven as nicely as intrauterine myocardial infarction ensuing from coronary arterial compression by a large rhabdomyoma. Echocardiographic research of patients with tuberous sclerosis reveal a high incidence of cardiac rhabdomyomas. Fenoglio and colleagues56 reported a 37% incidence of tuberous sclerosis of their autopsy series of patients with cardiac rhabdomyoma. However, a lot of their circumstances had been stillborns or newborns, and the analysis of tuberous sclerosis could additionally be troublesome in this age group. A retrospective examine in 33 infants and kids with cardiac rhabdomyoma collected from three pediatric cardiology facilities confirmed that 91% had tuberous sclerosis. This rivalry is further strengthened by the observation that in each of 5 infants, in whom fetal or early postnatal echocardiography revealed a cardiac tumor, tuberous sclerosis was subsequently diagnosed. However, the variety of rhabdomyomas steadily declined with follow-up, in order that by age 6 years, they utterly disappeared by echocardiography. Such biologic behavior helps the concept that cardiac rhabdomyomas, whether or not associated with tuberous sclerosis, could also be hamartomatous somewhat than truly neoplastic. The lesion has a definite predilection for the ventricles, with left ventricular involvement in virtually 100% and right ventricular involvement in roughly 80% of cases. Occasionally the lesions may grow to weird proportions, with intracavitary extension. The tissue consists of markedly swollen myocytes, showing almost "empty" cytoplasm with a centrally placed cytoplasmic mass and nucleus. Cytoplasmic strands prolong to the periphery of the cell, hence the term spider cell. The myocytes may appear fairly bizarre and typically reach monstrous sizes of up to eighty �m in diameter. The stromal element is usually scanty, though sometimes areas with distinct collagen might occur. The kind of polysaccharide concerned is rather labile (diastase sensitive), a striking contrast with that present in glycogen storage illness (diastase resistant). However, in the latter, the myocytes are normally not so massive, nor do they show the "spider" look, though they seem empty with a peripheral rim of myofibrils.
Order 30 gm himcolin with visa
The axial T2 picture (e) exhibits that this mass (arrow) is epidural in location erectile dysfunction caused by lipitor generic himcolin 30 gm visa, displacing the thecal sac to the proper erectile dysfunction treatment honey himcolin 30 gm order overnight delivery. An enhanced axial image (f) demonstrates the basic peripheral ring of enhancement typically seen surrounding a disc fragment (arrow) erectile dysfunction treatment brisbane generic 30 gm himcolin. While the situation on the sagittal picture (d) might need instructed a meningioma or schwannoma, each of these attainable tumors would have been intradural and proven homogenous enhancement, plus a schwannoma would have been hyperintense on the T2 pictures. The fissure is normally asymptomatic, although some consider that there could also be irritating substances secreted through it throughout its preliminary formation eight Radiology of the Spine for the Interventionalist ninety five. The enhanced fat-suppressed T1 image (b) demonstrates peripheral enhancement of the left lateral recess mass (arrow), typical of a disc fragment, with the thecal sac being the "second mass," displaced to the proper anteroposterior slippage, could also be predisposed as a outcome of congenital spinal stenosis. Neural Foraminal Narrowing � Due to a bulging disc that will or might not work together with nerve root which exits above the disc [25, 26]. While osteomyelitis/discitis can produce edema in the bone, there was no edema in the disc and no disc enhancement (not shown), typical of such a process. The axial T2-weighted image (c) shows a bulging disc with an annular fissure and moderate aspect hypertrophy, producing a mild diploma of central canal spinal stenosis eight Radiology of the Spine for the Interventionalist ninety seven. The sagittal T1 image (a) demonstrates low sign depth within the L5 and S1 our bodies representing edema, between which is a large anterior extrusion (arrow) from the L5�S1 disc. Kyphosis � Plain radiographs show the degree and site of kyphosis and end-plate irregularities. The axial picture (a) on the L4�L5 degree demonstrates severe degenerative side illness with a marked diploma of osteophyte formation along the best vertebral body margin (arrow, very low intensity), extending into the proper lateral recess to produce important compression of the best L5 nerve root. The sagittal view (b) demonstrates a grade 2 spondylolisthesis (arrow) secondary to the severe aspect disease. The left neural foramen is deformed by the slippage (c), and the exiting left L4 root (arrow) is compressed between the osteophytic aspects and the degenerated disc. The sagittal T2 sequence (a) shows the central canal throughout the lumbar backbone to be congenitally slim. The axial T1 picture (b) higher demonstrates the thickening of the ligamenta flava (arrowheads) secondary to the extreme aspect illness and the focal protru- sion (arrow) superimposed on the bulging disc. The T2 axial picture (c) demonstrates fluid within the degenerated aspect joints and the extreme compression of the thecal sac. Chronic Disc/Osteophyte Complex � Chronic disc bulging or protrusion stimulates osteoblasts to form an osteophytic ridge (disc/osteophyte complex) that protects towards further disc displacement. The sagittal-enhanced image (a) exhibits an epidural mass (arrow) extending from the disc house, surrounded by enhanced epidural tissue. The unenhanced (b) and enhanced (c) images at the similar L4�L5 disc area stage show the mass (arrows) to be a large disc fragment surrounded by enhancing scar tissue. There is intensive enhancing scar tissue surrounding the thecal sac in this patient who had undergone bilateral laminectomies. The fusion has resulted in altered pressures inside the close by discs, with subsequent degeneration. Uncinate spurring compresses the exiting nerve root, a typical explanation for higher extremity radiculopathy. Traumatic Injuries � Acute fractures � Lumbar [31] � Acute compression fracture 1. Nuclear Medicine bone scans could be misleading: 40% stay optimistic at 1 year and 10% at 2 years [13]. Laminectomies and bilateral pedicle screw fusion have been performed at the L4�L5 stage for a extreme grade 1 spondylolisthesis (0�25% slippage) because of degenerative facet illness (a). The axial T1 scan at the L3�L4 (b) level reveals the hypertrophied ligamenta flava (arrows), while the T2 scan (c) better shows the degenerated sides and disc, all combining to produce a reasonably extreme degree of central canal stenosis. The increased signal inside the cord is either edema, if acute, or gliosis, if continual eight. Involvement of anterior and middle columns (Denis classification), variable involvement of posterior columns. Type B: superior-posterior edge of vertebral body center column initiatives into canal. Type A (Chance fracture)-horizontal fracture by way of vertebral physique anteriorly and laminae/ sides posteriorly. The sagittal T2-weighted picture (a) exhibits a disc extrusion on the C3�C4 degree (arrow), elevating the posterior longitudinal ligament. Thin T2 gradient echo pictures at the C3�C4 neural foraminal stage (b, c) show a hyperintense disc extrusion (arrows) into the proper lateral recess and proximal proper neural foramen, obliterating visualization of the right C4 root; while that on the left is well seen. The increased sign throughout the disc fragment is indicative of its comparatively excessive water content material and thus its acute extrusion. The sagittal view (a) demonstrates a comparatively narrow cervical spinal canal, disc materials (arrow) protruding through an annular fissure at the C3�C4 disc area, and hyperintensity within the wire at and beneath the disc space level. The axial view (b) shows the disc protrusion to be broad-based; the annular fissure (arrow) to be fairly irregular, suggesting recent tearing; and the edematous spinal cord to be significantly compressed 2. Type B ("naked aspects")-horizontal fracture via the intervertebral disc and separation of the aspects posteriorly by way of ligamentous disruption. The forces required for acute fracture are a lot higher than for an acute cervical or lumbosacral fracture as a outcome of the rib cage holds the vertebrae in place; when there are such forces, fracture-dislocation and extreme neurological injury results. The left neural foramen is narrower than the right, secondary to osteophyte formation alongside the uncinate course of. The left C6 root is compressed, resulting in left arm pain in the C6 distribution. The hypointensity within the L1 body represents methylmeth- acrylate infused during earlier vertebroplasty. The axial image (b) via that stage demonstrates bony retropulsion (arrow) secondary to cephalocaudal (loading) forces, attribute of a burst fracture. On the sagittal T1 sequence (a), the mass is a combination of grey and white, whereas on the sagittal (b) and axial (c) T2 sequences, it also has combined white and gray colours, but in different places than on the T1 sequence. The evolution from oxyhemoglobin to deoxyhemoglobin and intracellular methemoglobin is way quicker than in a closed setting such as the mind. Once the hemorrhage has been exposed to room air, this conversion can occur within hours, not days. On T1, the grey of oxy- and deoxyhemoglobin is mixed with the white of early conversion to intracellular methemoglobin. The axial enhanced scan (b) reveals the intensive enhancing delicate tissue surrounding an abscess (arrow), extending into the left sacroiliac joint, S1 bony constructions, and left side joint promised patients; indium-111 and 99mTc-labeled leukocytes are very delicate in the remainder of the physique, however not the backbone as a end result of increased stress in disc. Imaging the Lumbosacral Spine for Radiculopathy � Need to detect nerve root compression. Abnormal veins are seen alongside the posterior cord surface before and after enhancement. Osteoporosis and multiplicity of fractures cut back the accuracy of bone scans within the detection of acute spinal and pelvic fractures. The bone scan remains constructive in 41% of sufferers at 1 yr, 10% at 2 years, and 3% at 3 years. The association between Modic changes and ache throughout 1-year follow-up in sufferers with lumbar radicular pain. The lumbar facet joint: a evaluate of present knowledge: part 1: anatomy, biomechanics, and grading. Morphologic and histologic research of the ligamentum flavum within the thoraco-lumbar area. Symptomatic spinal epidural lipomatosis after a single native epidural steroid injection. Reliability and validity of a new measurement of lumbar foraminal quantity using computed tomography. The sacroiliac joint: an outline of its anatomy, perform and potential medical implications. Anatomic buildings concerned in early- and late-stage sacroiliitis in spondyloarthritis: a detailed evaluation by contrast-enhanced magnetic resonance imaging. The relationship between the cervical spinal canal diameter and the pathological adjustments within the cervical spine. Anatomy and clinical vital of the uncinate process and uncovertebral joint: a complete review. Imaging of degenerative lumbar intervertebral discs; linking anatomy, pathology and imaging.
Discount 30 gm himcolin overnight delivery
History Historically erectile dysfunction zurich generic 30 gm himcolin with visa, ankle joint injections have been carried out blind or landmark guided; nevertheless impotence curse himcolin 30 gm order without a prescription, recent literature demonstrates the shortage of accuracy in comparison with smoking erectile dysfunction statistics generic 30 gm himcolin with amex image-guided techniques [42]. A frequent use of the intra-articular tibiotalar joint injection is supply of contrast for magnetic resonance arthrography to help delineate pathology within the ankle [42]. Side Effects and Complications Pathophysiology Rare unwanted aspect effects embody skin atrophy and dystrophic joint calcification at the knee. Two of the most typical causes for tibiotalar joint pathology are osteoarthritis and rheumatoid arthritis. Other illness processes embrace psoriatic arthritis, gout, and seronegative spondyloarthropathies. At the ankle, accidents or fractures are the most typical etiology of osteoarthritis [43, 44]. Rheumatoid arthritis is an autoimmune disease affecting the synovium of the joints leading to progressive and painful joint destruction. Small joints are the most commonly affected joints; nonetheless, any synovial joint can be involved. Diagnosis Refer to previous sections for additional particulars of diagnosing osteoarthritis. Diagnosis of rheumatoid arthritis is generally accomplished via the presence of rheumatoid factor, though extra sensitive and particular serological tests may be used [45]. Additional confirmation can be carried out with plain movie radiographs of affected joints with characteristic findings of soft-tissue swelling, bony erosions, and lack of joint space. Smoking is essentially the most modifiable risk factor associated with rheumatoid arthritis [45]. Relevant Anatomy [18] the ankle joint is a hinged synovial joint created by the articulation from the distal finish of the tibia, fibula, and the superior aspect of the talus. The primary movement at the ankle joint is dorsiflexion and plantar with end motion restriction due primarily to bony abutment. Muscles/Tendons/Ligaments the muscle tissue that cross the ankle joint within the anterior airplane are the tibialis anterior, extensor hallucis longus, and extensor digitorum longus. They are held in plane transversely by the superior and inferior extensor retinacula. Evidence Base the accuracy of landmark-guided injections throughout the literature ranges from technique of 64% to 88%, whereas ultrasoundguided injections have been discovered to be 100% accurate in a number of research with stage 2 proof [9, 41, 46, 47]. Fluoroscopic guided injection accuracy has not been studied as extensively but is felt to be an acceptable technique of steerage for injections. Accuracy is a crucial factor when considering the use of injections for placement of contrast for subsequent magnetic resonance arthrography [49]. The major medications delivered through intra-articular ankle injections are corticosteroids, anesthetics, and viscosupplementation. The efficacy of corticosteroids for tibiotalar joint injections has a positive development with level 4 evidence according to a current evaluation by Finnoff et al. It is common apply to not give more than 3 corticosteroid injections over a 12-month interval. Viscosupplementation is mostly given as a sequence of injections and could be repeated every 6 months. Within the limited literature on the topic, no significant variations have been discovered between the two major approaches to the tibiotalar joint � anteromedial versus anterolateral [49, 55]. In the presence of joint space narrowing, the anteromedial strategy may be difficult, and so the lateral mortise approach could additionally be of utility [49, 57]. Neurovasculature Anteriorly the deep peroneal nerve and the anterior tibial artery course throughout the joint between the extensor digitorum longus and extensor hallucis longus descending into the dorsal side of the foot. Interventional Technical Aspects Refer to the earlier section for common preinjection patient dialogue, schooling, and postinjection care. Putting the ankle into plantarflexion may help to open the joint area or expose neurovasculature. Preparation � Sterile gloves � Sterile probe cover and gel if utilizing ultrasound � Skin prep � chlorhexidine, alcohol, and/or Betadine options � 25 gauge needle 1. If meeting resistance or hitting bone, retract and readjust with out removing the needle from the pores and skin. The anterior tibiofibular ligament and anterior talofibular ligament are above and beneath the target injection website, respectively. Lateral Mortise [49, 57] � Position affected person supine with the ankle in slight plantarflexion. Common indications for injecting the ankle joint are symptomatic osteoarthritis and rheumatoid arthritis, in addition to prognosis of pathology. Favorable development for corticosteroids and reasonable proof for viscosupplementation. Ankle joint injections have improved accuracy with fluoroscopy and ultrasonography. Anterolateral may be useful when important medial joint space narrowing is present. Intra-articular hip injections using ultrasound steering: accuracy using a linear array transducer. Ultrasound-guided hip injections: a comparative research with fluoroscopy-guided injections. Dramatically elevated musculoskeletal ultrasound utilization from 2000 to 2009, especially by podiatrists in non-public offices. Office-based ultrasound-guided intra-articular hip injection: technique for physiatric practice. Risk components for the event of hip osteoarthritis: a population-based prospective research. Symposium: proof for the use of intra-articular cortisone or hyaluronic acid injection within the hip. The symptomatic effects of intra-articular administration of hylan G-F 20 on osteoarthritis of the hip: scientific information of 6 months follow-up. A evaluation of viscosupplementation for osteoarthritis of the hip and a description of an ultrasound-guided hip injection technique. Development of a scientific prediction rule for diagnosing hip osteoarthritis in individuals with unilateral hip pain. Relationship of peak, weight and body mass index to the danger of hip and knee replacements in middle-aged women. Side Effects and Complications � Neurovascular issues are unlikely to happen if the nearby vessels are palpated and marked prior to injection. The most typical causes to perform intra-articular hip procedures is for joint aspiration, prognosis of pathology, and therapy of ache associated with osteoarthritis. The literature for ortho-biologics and viscosupplementation is encouraging, however more studies are needed. Fluoroscopic or ultrasound guidance is recommended for a safe and effective injection. Intra-articular corticosteroid injections have been shown to lower ache within the acute part following exacerbations of osteoarthritis or rheumatoid arthritis. Viscosupplementation has been proven to reduce knee pain for as a lot as 26 weeks and might help delay knee replacement in select sufferers. The superolateral method to anatomically guided intra-articular knee injections has been proven to be essentially the most accurate. Ultrasound guidance considerably improved the accuracy of intra-articular injections of the knee in comparison with anatomical steering. Epidemiology of ankle arthritis: report of a consecutive sequence of 639 patients from a tertiary orthopaedic heart. Ultrasound-guided versus nonguided tibiotalar joint and sinus tarsi injections: a cadaveric research. Ultrasound versus anatomic steerage for intra-articular and periarticular injection: a scientific evaluation. Viscosupplementation of the ankle: a potential research with an average follow-up of 45. Sodium hyaluronate within the treatment of osteoarthritis of the ankle: a controlled, randomized, double-blind pilot research.
| Comparative prices of Himcolin |
| # | Retailer | Average price |
| 1 | Giant Eagle | 853 |
| 2 | Amazon.com | 475 |
| 3 | Belk | 813 |
| 4 | Best Buy | 368 |
| 5 | Ruddick Corp. | 699 |
| 6 | Kohl's | 630 |
| 7 | H-E-B | 417 |
| 8 | Ross Stores | 499 |
Purchase 30 gm himcolin mastercard
On the opposite hand erectile dysfunction market buy himcolin 30 gm fast delivery, rheumatoid arthritis is an autoimmune systemic inflammatory illness affecting the synovium of the shoulder joint viagra causes erectile dysfunction buy himcolin 30 gm on line. Although shoulder involvement usually happens late in the middle of the disease erectile dysfunction drugs medicare cheap himcolin 30 gm, shoulder involvement is pretty frequent in rheumatoid arthritis. This is normally chronic in nature, related to periodic exacerbations secondary to irritation. The earliest adjustments include narrowing of the articular cartilage and inferior glenoid fossa irregularities. However, in advanced disease, a large spur may be evident along with flattening of the humeral head and obliteration of the articular cartilage on the inferior glenoid. However, oftentimes, correlation with symptomatology and scientific examination may not always be evident. However, after failed conservative administration, intra-articular injection with glucocorticoids or a collection of injections with sodium hyaluronate could present some aid from shoulder ache. Injection of the glenohumeral joint could be carried out from an anterior and posterior strategy. The affected person is normally sitting comfortably with the arm resting at the side and the shoulder externally rotated. Anatomic landmarks embody the pinnacle of the humerus, coracoid process, and the acromion. Glenohumeral Joint this is essentially the most cellular joint within the body representing the articulation of the humerus and the glenoid fossa. This joint is stabilized by ligaments (joint capsule, labrum, and glenohumeral ligaments) and muscles that embody the rotator cuff (supraspinatus, infraspinatus, teres minor, and subscapularis). Indications the major indications for such injection embody osteoarthritis, adhesive capsulitis (frozen shoulder), and rheumatoid arthritis [19�25]. Note the distinction circulate into the joint cavity along the glenoid fossa Standard sterile technique must be followed at all times to decrease the chances of an infection which could be catastrophic. Anterior Approach the needle is inserted 1 cm lateral to the coracoid course of simply medial to the pinnacle of the humerus. If the needle gets contact in opposition to bone, it ought to be redirected in a different angle. Posterior Approach the purpose of needle entry is approximately 2�3 cm inferior to the posterolateral corner of the acromion. After standard aseptic technique, a needle is introduced by way of the skin with an in-plane method from the lateral shoulder with a medial trajectory. The goal for the needle position is the posterior humeral head near the posterior labrum. Care is made to keep away from injuring the labrum or the articular floor of the humerus. Elbow Joint Introduction Elbow pain could also be attributed to ache generators originating from the joint itself and surrounding constructions corresponding to muscle and ligaments or to referred ache from the neck or the shoulder. Fluoroscopic-Guided Glenohumeral Joint Injection the affected person is positioned supine on the table. The last goal for the needle can be within the joint or along the superior-medial portion of the humeral head. Injection of contrast ought to show easy flow throughout the joint capsule which may additionally define the biceps tendon sheath. After affirmation of needle placement, treatment also wants to be injected with out much resistance. Pathophysiology Elbow pain entails pathologic alteration within the musculotendinous origins of the extensor or flexor tendons on the lateral and medial epicondyles. The affected structure reveals edema and fibroblast proliferation within the subtendinous house, tendinopathy with hypervascularity, and spur formation with a sharp longitudinal ridge on the medial and lateral epicondyles [28]. Ultrasound-Guided Glenohumeral Joint Injection the affected person is positioned lateral recumbent with the affected shoulder up. Scanning of the posterior shoulder is performed with the transducer in a transverse indirect airplane to demonstrate Evidence Base In a evaluation by Stephens et al. The main movement is supination and pronation at the articulation that allows rotation from 0� to 180�. The common source of pain is the epicondyles that can simply be palpated on the medial and lateral sides of the distal humerus. Also, the elbow joint is surrounded by a quantity of bursae, and swelling may occur, inflicting pain. Ulnar and median nerves course thought the elbow joint that may be impinged inflicting entrapment syndrome. Examination of the elbow joint requires assessment of the vary of motion (flexion, extension, pronation, and supination). Palpation of the lateral and medial epicondyles to determine tendinopathies and determine the presence of effusion and focal tenderness and olecranon bursa for swelling and thickening would enable analysis of elbow joint pathology. Repetitive actions of the elbow that exceed tissue capability could also be a cause of epicondylitis in each lateral and medial epicondyles. Gouty arthritis could involve the olecranon bursa and may be the initial presentation of gout. Since the elbow is a non-weight-bearing joint, degenerative adjustments are often uncommon [30]. Narrowing or loss of joint space and osteophytic modifications are consistent with osteoarthritis. Palpation of surface landmarks contains the delicate tissue on the middle of the triangle fashioned by the olecranon, head of the radius, and lateral epicondyle. The injection should be gradual and clean with none resistance upon injection beneath fixed pressure. Females are generally affected than males with approximately 3 to 1 ratio [31, 32]. Interventional Technical Aspects Identification of the flexor carpi radialis and palmaris tendon on the wrist is necessary. Using a 25-gauge needle, make a pores and skin wheal with lidocaine simply medial to the palmaris longus tendon and roughly 1 cm proximal to the wrist crease. Using the same gauge needle, direct it toward the third digit at a 30� angle and advance to 1. Aspirate to verify for intravascular placement earlier than injection of glucocorticoid, and it must be smooth with minimal to no resistance. Acquired or congenital structural changes of the carpal tunnel may outcome within the impingement of the median nerve. The lowest carpal tunnel strain is seen when the wrist is in a impartial or barely flexed position, and it will increase proportionately with deviation from this posture as seen with computer use [35, 37, 38]. Ultrasound-Guided Carpal Tunnel Injection Ultrasound-guided injection is often done to avoid direct trauma to the median nerve. A high-frequency linear probe is positioned in a transverse place throughout the carpal tunnel. The needle tip ought to pierce the transverse carpal ligament to enter the carpal tunnel. Easy flow of injectate ought to show hydrodissection of the median nerve away from the flexor tendons on the needle goal web site near the median nerve. In conclusion, an intensive historical past and physical examination are warranted previous to any kind of intra-articular injections. A good grasp on anatomy and utilization of various imaging modalities improve outcome and success rate of such injections. Evidence Base Two good-quality randomized managed trials have shown that corticosteroid injections have been clinically simpler than placebo and oral corticosteroid in a 4-week period [39, 40]. Indications and Diagnosis the carpal tunnel is fashioned by the flexor retinaculum superiorly and eight carpal bones inferiorly [42]. The median nerve programs underneath the transverse retinaculum and could also be compressed as it travels via the carpal tunnel. Anatomic compression can be caused by thickening and irritation of the flexor tendons as they cross through alongside the median nerve. It is a scientific analysis, and crucial feature is nocturnal pain and paresthesia alongside the nerve distribution [36].
30 gm himcolin generic fast delivery
Following the incision erectile dysfunction treatment natural way buy himcolin 30 gm low cost, an axe is used to make an entry gap in the proximal metaphysis of the tibia yellow 5 impotence 30 gm himcolin purchase with amex, through which a guide wire is launched erectile dysfunction yoga youtube purchase 30 gm himcolin with amex. The information wire is positioned throughout the aligned fracture, and the nail is launched and driven over the guide wire. Before nail insertion, the medullary canal usually is reamed to permit use of a bigger nail. Most nails are interlocked each proximally and distally with screws that cross from the bone through holes in the nail. Stainless steel pins are drilled into the proximal and distal fragments of the fracture via stab wounds within the skin and subcutaneous tissues. Pin clamps and an exterior frame are hooked up and the fracture aligned with the assistance of the I. Following fracture alignment, the pin clamps and frames are tightened to hold fracture alignment. Wound irrigation and debridement usually accompany software of the fixation frame. A longitudinal incision is made over the fractured medial and/or lateral malleoli. Dissection is carried instantly down to the bone, and the fracture is identified and lowered under direct vision. The fractures are realigned underneath direct vision and stuck and stabilized with pins, plates, and/or screws. The fracture is mobilized, normally grafted with autogenous or allograft bone, and realigned. With an anterior strategy, a longitudinal incision is made anteromedial or anterolateral to the shaft of the tibia. If the tibia is approached with a posterolateral incision, the patient is turned susceptible and a longitudinal incision is made just posterior to the fibula. Dissection is carried down posteriorly to the interosseous membrane, to the tibia, and the process turns into identical to the anterior strategy. In the case of a malunion, the bone may be osteotomized with a saw or osteotomes to enable realignment. If skeletal fixation is used, a plate could additionally be attached to the bone through the identical incision. Alternatively, an intramedullary nail could additionally be placed through an incision anterior to the tibial tubercle. If an intramedullary device is used, the canal may be reamed with intramedullary reamers prior to placement of the nail. A third sort of skeletal fixation is the exterior fixator that stabilizes the nonunion via percutaneous pins positioned into the proximal and distal tibia, which are then spanned by a device with pin clamps at each ends. An intraop x-ray is often used to confirm fixation and placement of gadgets; alternatively, an I. Variant process or approaches: Autogenous bone grafting from the iliac crest is usually used to stimulate therapeutic. An incision is made instantly over the iliac crest, and muscular tissues are stripped from the crest and table of the ilium. Osteotomes and gouges are used to remove both the inside or outer desk of the ilium and cancellous bone between the two tables. The ankle joint usually is inspected via anterolateral and anteromedial portals (entry wounds). If the ankle joint is tight, a mechanical distractor (external fixator distraction apparatus spanning the ankle joint) may be used. The distractor is connected to the bones by way of percutaneous pins, as within the case of the applying of an external fixator. The joint often is opened with an anterolateral midline or anteromedial longitudinal incision. Tendons and neurovascular constructions are fastidiously retracted to expose the joint capsule, which is then opened consistent with the skin incision. After intraarticular pathology is addressed, cautious closure of the capsule is carried out, taking care to acquire good hemostasis. The ankle joint is uncovered, and the surfaces of the joint are debrided either with osteotomes or a burr. Cancellous bone is uncovered on the distal tibia and talus, and the joint is clamped together either with a simple exterior fixation system with pins going by way of the distal tibia and talus, or with bone screws that go from the distal tibia into the talus. An incision is made posterior to the distal fibula, curving around the lateral malleolus and ending in the anterolateral foot. The peroneus brevis tendon is identified and indifferent from its musculotendinous junction within the leg, and the peroneus brevis muscle is sutured to the peroneus longus tendon. A hole is drilled from anterior to posterior in the distal lateral malleolus; then the indifferent end of the peroneus brevis tendon is threaded through the outlet. It is then hooked up to either the calcaneus or the talus, anterior to the lateral malleolus, with a staple or by suturing into a gap in the bone. It is more practical than below-knee amputation because patients can bear weight on the top of the stump; nonetheless, success is poor in sufferers with vascular illness or peripheral neuropathy. The posterior flap is dissected immediately from the calcaneus, carefully preserving the robust heel pad and its blood provide. The heel pad is sutured directly to the distal tibia to prevent migration and to cover the bone finish. The posterior flap is then sutured to the anterior flap with interrupted sutures and a compression dressing utilized. A transverse dorsal incision is made at the transmetatarsal degree, and a plantar incision is made beginning at the corners of the dorsal incision and increasing distally to the metatarsal heads to create a long plantar flap. The plantar flap is reflected proximally to the midmetatarsal degree and tapered distally. The metatarsals are sectioned with a noticed, and nerves and tendons are sectioned proximal to the osteotomies. The plantar flap is then introduced over the ends of the bones and sutured with interrupted sutures to the dorsal flap. Variant procedure or approaches: Other partial-foot amputations, corresponding to midtarsal and ray amputation, are much much less common. For tendon lengthening, a longitudinal incision usually is made instantly over the tendon. Subcutaneous tissues and tendon sheath are incised to expose the tendon, which is transected with a Z-type incision. The tendon is positioned in its lengthened position, and the ends of the Z are closed with absorbable suture. In a tendon transfer, the tendon usually is minimize near its insertion and transferred to a model new bony insertion, which often requires a separate incision. The tendon is hooked up to the bone either with a steel staple or by suturing it into a drill hole in the bone. Variant process or approaches: Achilles tendon lengthening is used to convey the ankle out of equinus. A posterior tibial tendon lengthening and/or posterior ankle capsulotomy may accompany the process. The most commonly carried out stumps incorporate anterior and posterior flaps of equal size. The underlying muscle tissue (hamstrings and quadriceps) are both sewn to each other (myoplasty) or to bone (myodesis). This is a multistage process used for soiled, traumatic amputations, infection, or above-knee amputations with questionable survival and often is completed as a lifesaving measure. Internal fixation of a part of the remaining femur may be indicated in traumatic amputations. The condition of the soft tissues might dictate the extent and/or type of flaps used. A lengthy posterior flap, which is 2�3 times the diameter of the leg in size, is then made. The bone is uncovered anteriorly, and the anterolateral neurovascular constructions and muscle tissue are transected and ligated as applicable. The bone is then transected with a bone noticed, and the posterior buildings are transected and ligated as applicable. The amputated leg and foot are then removed from the table, and the posterior flap is tapered and shaped for closure. Finally, a drain is positioned (sometimes), and both a compression dressing or an instantaneous postop solid is applied.
30 gm himcolin sale
Disma N erectile dysfunction best treatment order himcolin 30 gm with visa, Astuto M erectile dysfunction statistics us generic himcolin 30 gm on-line, Rizzo G what age does erectile dysfunction usually start himcolin 30 gm buy cheap line, et al: Propofol sedation with fentanyl or midazolam throughout oesophago-gastroduodenoscopy in children. Each set of knowledge takes 2�3 min to collect, permitting many children to complete scans with none sedation. Techniques include inhalational anesthesia and/or steady infusion of propofol (100�200 mcg/kg/min), and remifentanil (0. Objects could be propelled towards the magnet with adequate velocity and force to end in critical or fatal harm to the affected person and/or well being care supplier. De Sanctis Briggs V: Magnetic resonance imaging beneath sedation in newborns and infants: a study of 640 cases utilizing sevoflurane. Venous blood is withdrawn by gravity by way of a servoregulator to stop pump from actively siphoning venous return. A pump delivers blood back to the arterial cannula after it passes by way of the membrane oxygenator and heat exchanger. Venous return is from the right atrium, whereas arterial infusion is into the aortic arch in double-cannula (venoarterial) or right atrium (venovenous) techniques. Vascular access is accomplished with one (venovenous) or two (venoarterial) cannulas. Successful management of these patients includes meticulous planning, complete teamwork, communication, and a focus to element. Intrahospital transport of these patients often requires multiple personnel from varied medical specialties, and therefore, it is essential to elect a staff leader prior to transport and to allocate particular tasks. The plastic elements of the bypass circuit can sequester varying amounts of the intravenous agents, especially fentanyl, altering the plasma ranges and resulting in unpredictable hemodynamic changes. Anesthetic brokers trigger preload and afterload modifications and subsequently further volume (blood products and colloids) and vasoactive agents should be available to find a way to keep adequate filling and blood stress. The potential detrimental results of diaphragmatic restore on respiratory perform could be managed with increased circuit circulate. The procedures described in this chapter are but a small sampling of the methods by which anesthesia is utilized in medical/dental workplaces. Although anesthesia practiced in an workplace carries the identical risks, burdens of duty, and ability requirements as in a fully equipped surgical center, within the office setting, the anesthesiologist could additionally be anticipated to organize for the oxygen supply, suction, monitoring, and emergency equipment. This distinctive challenge for the anesthesia provider contains working with personnel unfamiliar with anesthesia concerns, converting the office right into a facility acceptable for anesthesia, selecting appropriate patients, providing protected and efficient anesthesia/analgesia, and properly preparing and recovering the sufferers. In California, for example, dental workplaces are regulated in a unique way than medical offices. For many years, the California Dental Board has regulated anesthesia within the dental or oral surgery workplace by credentialing the anesthesia provider and/or the office facility itself. The Dental Board additionally issues "Conscious Sedation" permits to these dental practitioners who qualify and wish to use this technique. A precordial stethoscope is kind of helpful for monitoring respirations, particularly in the dental affected person, in whom airway obstruction is a frequent prevalence in the course of the process. In the credentialed medical (nondental) facility, these things are required to be on website. It is the responsibility of the anesthesia supplier to make certain these things are available within the medical or dental facility earlier than administering an anesthetic. The patient undergoing full face laser resurfacing will most probably require deep sedation or general anesthesia because this process can be fairly painful. In the office setting, the ability to achieve a successful end result relies to begin with on acceptable affected person selection. A written packet describing some of this info can be given to the patient upfront. Safe and accepted npo necessities on the day of the process are as follows: � A gentle breakfast. They should still really feel drowsy, but this could not forestall them from with the ability to walk with assistance. Discharge directions concerning appropriate postop activities should be given to the responsible grownup with the patient. The anesthesiologist also ought to give the responsible party (parent, good friend, different relative) his/her pager or cellular phone quantity in the occasion they need to contact the anesthesiologist after patient discharge. American Society of Anesthesiologists: Continuum of Depth of Sedation, Defnition of General Anesthesia and Levels of Sedation and Analgesia. Berman Description: A number of medical gadgets have been approved for use to enhance skin concerns, similar to wrinkles, precancerous pores and skin lesions (actinic keratoses), discoloration, acne scars, traumatic scars, and sagging pores and skin. This process yielded great outcomes, but extensive heat from this process caused some undesirable unwanted effects similar to scarring or pigmentation issues, prompting the business to develop the cooler and extra conservative resurfacing tool utilizing the erbium laser. Less than a decade later, a novel fractionated laser resurfacing device was developed that removed only a fraction of the pores and skin in a sample reminiscent of pixels in newspaper print. Certainly, the dangers and side effects were reduced in comparability with the older know-how, though this more conservative method rendered a more modest enchancment of pores and skin considerations. Further analysis led to the event of nonablative technologies such as radiofrequency/ ultrasound/nonlaser light-based devices, most of which resulted in higher side impact profiles and optimistic outcomes. Although the holy grail of units would render a no-down-time, painless process void of adverse results, the seek for such continues to elude us. Meanwhile, physicians who perform these procedures should encourage sufferers to go for office-based anesthesia and thus make the experience a extra nice one for all involved. After a Betadine prep, anesthetic eye drops are used, adopted by the insertion of protective corneal shields. The treatment then begins with one or more passes performed at various energy levels. Usual preop analysis: Wrinkles, precancerous pores and skin lesions (actinic keratoses), pimples scars, and traumatic scars. All dental caries are removed, the restorations are placed, and all debris is irrigated and suctioned away from the rubber dam, which is then eliminated. After the operative phase of therapy is completed, the next therapy phases proceed. After the therapy is completed, the dentist examines the mouth and removes any free gauze, debris, or other materials left over from the remedy earlier than the anesthesiologist begins the method of emergence from anesthesia. Examples embody a 20-mo-old youngster with early childhood caries, an 8-yrold autistic youngster, or a child of any age with cerebral palsy, obesity, Down syndrome, or different congenital syndrome. These patients must be screened upfront for clinical conditions that might put them in danger for issues intraop or postop. Specifically, a patient with any cardiac, respiratory, endocrine, or neurologic downside have to be evaluated. Examples of such conditions embody mild nonsteroid-dependent bronchial asthma, corrected congenital coronary heart disease, or a steady Sz dysfunction. Following sedation, the patient is positioned in the dental chair, with the pinnacle positioned to maintain an open airway. A nasal airway is positioned with care (to keep away from epistaxis) after the dental x-rays are taken. The anesthesiologist have to be continually vigilant in sustaining an open airway in these sufferers within the face of an oral process. Dental implants are inserted surgically into the mandibular or maxillary alveolar bone the place tooth are lacking. Single implants may be carried out with local anesthesia, however multiple or complicated procedures are best accomplished with iv sedation. After the native anesthetic is administered, a mucoperiosteal flap is raised over the edentulous alveolus, and the bone is uncovered. Precise drill holes are made within the bone, and the implants are screwed or tapped into place. Bone grafting may be needed across the implants to fill in defects and is carried out using autologous, allogenic, xenogenic, or synthetic supplies. The bone is allowed to heal across the implant, and 2-6 mo later the implant can be utilized to attach crowns, bridges, or dentures. Most minor grafting procedures are accomplished within the dental workplace underneath iv sedation and local anesthesia. The anesthesiologist ought to be consulted in advance about these sufferers so that questions about their medical situations can be answered and a current list of medicines may be obtained. If continual medical situations are secure, sufferers usually can obtain "acutely aware sedation" and monitoring by the anesthesiologist for this process within the workplace. In the grownup patient having dental implants, the maintenance of a frivolously sedated state is achieved using a combination of iv midazolam, fentanyl (or meperidine), and small amounts of ketamine (20�30 mg/dose).
30 gm himcolin purchase with mastercard
Periprocedural anticoagulation � Adult � Inpatient and Ambulatory� Clinical Practice Guideline erectile dysfunction pump how to use purchase himcolin 30 gm free shipping. Percutaneous Lumbar Thermal Annular Procedures Standiford Helm 16 Introduction the intervertebral disc is a common source of low again ache erectile dysfunction pills online himcolin 30 gm purchase with mastercard. The disc is the cause of roughly 25% of circumstances of persistent low again ache treatment of erectile dysfunction using platelet-rich plasma cheap himcolin 30 gm with mastercard, with estimates ranging from 17% to 42% [1�3]. Once current, pain from the intervertebral disc persists in as a lot as 80% of patients [4]. On a physiologic basis, the event of tearing in the annulus, with subsequent neovascularization and development of nerves from the outer annulus to the inside annulus and irritation of these nerves by inflammatory elements associated with therapeutic, remains the most engaging hypothesis [6]. Alternative theories are that the warmth shrinks the collagen, inflicting it to reorganize and strengthen, or that granulation tissue is cauterized [7]. Fusion of the adjacent vertebral bodies has commonly been used, with minimal profit for this prognosis [9, 10]. Lumbar epidural injections provide significant benefit in ache and performance in discogenic ache [11]. Various injection therapies, together with ozone, methylene blue, and various biologic preparations, have been tried and show early promise [12�14]. Identifying the intervertebral disc because the source of low back pain may be troublesome. History By the early Nineteen Nineties, there was considerable interest in the use of heat to deal with discogenic low again ache. In 1993, Eric Cosman, who first conceptualized the application of radiofrequency power to generate warmth in tissues, and Menno Sluijter, who pioneered the clinical application of radiofrequency, utilized for a patent to use radiofrequency energy applied to the nucleus, not the annulus, to treat low back pain [17]. Radiofrequency waves, between 250,000 and a 1,000,000 Hertz, trigger ionic heating in the tissue instantly adjoining to the electrode. Tissue ablating heat is generated by ions shifting in response to the radiofrequency electromagnetic field. This ionic activity causes both the tissue and the thermistor in the radiofrequency probe to heat up [18]. They rejected radiofrequency as being unable, with then available know-how, to apply enough warmth across the annulus to create the desired lesion. They rejected laser warmth for lack of control and the chance to adjoining neural tissue. They chosen conductive heating, which is done by heating a wire, which transfers heat to the fluids in the adjoining tissue, which in flip heats the target tissue. Patient selection required failure of conservative remedy, ache restricted to the low back with no neurologic involvement of the decrease extremities, disc height of a minimum of 50% of normal, and optimistic discography at a level with a documented annular tear. The normal heating protocol was to enhance the temperature of the probe to 90� C over 13 min and keep the 90� temperature for four min. The monitor photographs and generator noises of an actual procedure have been then displayed, in order that the placebo affected person had the same intra-procedural expertise as patients present process the procedure. Of the 64 participants, 8 were excluded from that study for varied protocol violations. With a number wanted to deal with of 5 to get a 75% reduction in scores, they concluded that it was a worthwhile intervention for chosen sufferers. At the tip of the procedure, all patients got one hundred mg of cefazolin intradiscally. Further, placebo results are anticipated in studies; the absence of one raises methodological questions [36�38]. The introducer is placed in the posterior annulus, using fluoroscopic and impedance monitoring, and the catheter is then handed alongside the posterior aspect of the annulus as proven in. A lesion is then made using radiofrequency power utilized over 10 min, with a maximum temperature of 65� C. Biacuplasty A limiting consider using radiofrequency is that because the ionic heating of the tissues heats up the radiofrequency electrode, the tissue immediately adjoining to the electrode turns into heated, leading to charring, increased impedance, and limitations on lesion measurement. Using water to cool the electrode prevents the charring adjacent to the electrode and permits a big lesion side. Both Pauza [42] and Petersohn 16 Percutaneous Lumbar Thermal Annular Procedures 303. A bipolar lesion is made throughout the posterior annulus at 50 �C for 15 min followed, without transferring the electrodes, by monopolar lesions at 60� for 2 min and 30 s. Inclusion standards were low back pain unresponsive to conservative care, disc height of at least 50% and concordant discography in diseased discs with regular discography in control discs. They excluded sufferers with more than two involved ranges or with a historical past of any previous lumbar spine surgery, disc bulges higher than 5 mm, or structural abnormalities corresponding to spondylolisthesis or central canal stenosis. They found six reviews of nerve root harm, 5 of which have been associated to the introducer needle placement. A separate report described a case of catheter shearing in which the catheter migrated from the annulus to the epidural area, inflicting nerve root irritation and necessitating surgical removing [47]. Discitis, osteonecrosis, and the event of grade 1 anterolisthesis have been reported [23, 50]. In one case, the catheter was positioned within the vertebral foramen, a gross violation of ordinary of care, so that the cauda equina was directly heated; in the second, the catheter was evidently appropriately placed [53]. The precise radiofrequency conductor containing the thermocouple (yellow) is accompanied by the cool water inlet (green) and outlet (red) (From Ball [18], with permission) eased, fissured annulus. The solely complication reported with biacuplasty is the anticipated transient low back pain after needle insertion [54]. If the ache persists after conservative therapy, including therapy, exercise, oral and topical medications, and epidural injection remedy, treatment choices are restricted, and in the absence of other therapies, the situation is unlikely to enhance. Surgical procedures present unsure outcomes and have significant dangers and morbidity, together with major decrements in operate. Isotherm lines kind dumbbell form around and between radiofrequency probes to cover the posterior section of the annulus fibrosus (Adapted from Kapural et al. Tearing of the annulus can lead to decreased impedance with warmth lesions extending to the region of the motor rootlets. Evidence-informed management of chronic low back ache with intradiscal electrothermal therapy. Intradiscal electrothermal therapy for chronic discogenic low back ache: a prospective consequence examine with minimum 1-year follow-up. Systematic evaluate of randomized trials evaluating lumbar fusion surgery to nonoperative look after therapy of persistent again pain. Fusion surgical procedure for lumbar degenerative disc illness: still more questions than answers. A randomized, double-blind, active-controlled trial of fluoroscopic lumbar interlaminar epidural injections in chronic axial or discogenic low back ache: results of 2-year follow-up. Ozone remedy as a treatment for low again pain secondary to herniated disc: a systematic evaluate and meta-analysis of randomized controlled trials. A randomized placebo-controlled trial of intradiscal methylene blue injection for the therapy of continual discogenic low back ache. Rejuvenation of nucleus pulposus cells utilizing extracellular matrix deposited by synovium-derived stem cells. The science of typical and water-cooled monopolar lumbar radiofrequency rhizotomy: an electrical engineering point of view. Randomized controlled trial of percutaneous intradiscal radiofrequency thermocoagulation for persistent discogenic back ache: lack of effect from a 90-second 70 C lesion. Percutaneous therapy of painful lumbar disc derangement with a navigable intradiscal thermal catheter: A pilot study. Paper introduced at: Proceedings of the 13th Annual Meeting of the North American Spine Society, San Francisco, 1998. A randomized, placebocontrolled trial of intradiscal electrothermal therapy for the remedy of discogenic low again pain. A randomized, double-blind, controlled trial: Intradiscal electrothermal remedy versus placebo for the therapy of continual discogenic low back ache. Intradiscal electrothermal remedy within the treatment of persistent low again pain: expertise with 93 sufferers. Intradiscal electrothermal annuloplasty remedy: a case sequence research resulting in new concerns. Risk elements for failure and complications of intradiscal electrothermal therapy: a pilot research.
Buy 30 gm himcolin mastercard
Abnormal brain chemistry in chronic again ache: an in vivo proton magnetic resonance spectroscopy study erectile dysfunction drugs nz generic 30 gm himcolin amex. Unilateral lower in thalamic exercise observed with positron emission tomography in patients with persistent neuropathic pain erectile dysfunction under 35 himcolin 30 gm buy cheap line. Neuropsychological evaluation of continual non-malignant pain sufferers handled in a multidisciplinary pain center what causes erectile dysfunction cure purchase himcolin 30 gm with visa. Functional morphology of nociceptive and different nice sensory endings in different tissues. Na+ channel accumulation on axolemma of afferent endings in nerve end neuromas in Apteronotus. Injury type-specific calcium channel 2-1 subunit up-regulation in rat neuropathic ache models correlates with antiallodynic effects of gabapentin. Characterization of [3H]gabapentin binding to a novel web site in fee brain: homogenate binding research. Glutamate pharmacology and metabolism in peripheral major afferents: physiological and pathophysiological mechanism. Pregabalin rectifies aberrant brain chemistry connectivity, and practical response in continual ache patients. Peripheral axonal injury leads to reduced mu opioid receptor pre- and post- synaptic action in the spinal wire. Dose-response relationship of opioids in nociceptive and neuropathic postoperative ache. Pharmacology and Clinical Relevance of Commonly Used Drugs Natalia Murinova, Daniel Krashin, and Alan D. Kaye three Introduction Many interventional ache procedures involve the usage of drugs. The practitioner should know the properties of the medications intimately, with their benefits and risks. It is noteworthy that virtually all clinical studies exclude sufferers with critical medical conditions and polypharmacy. Pain sufferers in follow are sometimes medically complex and take quite a few prescription medicines and dietary supplements. Both suppliers and patients have to be educated to understand the benefits, alternatives, and potential side effects of therapies on this complex setting. Local Anesthetics Early Spanish accounts describe the Andean peoples chewing coca leaves to decrease starvation, enhance vitality, and numb the ache of toothache [1]. Karl Koller, an ophthalmologist, discovered of cocaine from Sigmund Freud and, in 1884, was the primary to use cocaine as a neighborhood anesthetic for surgery [1]. All native anesthetics take effect through the reversible inhibition of sodium channels on neuronal membranes, which disrupts nerve sign transmission [2]. Local anesthetic molecules have three distinct useful components: an fragrant ring, an ester or amide residue, and an amine group. Within the body, a number of the molecules change to the un-ionized type, which is lipophilic and enters nerve membranes. Each native anesthetic has a particular pKa value, outlined because the pH at which half the molecules are ionized. Higher pKa values imply that more molecules stay ionized on the physiological pH of 7. Inflamed or infected tissue turns into extra acidic, which can result in decreased effectiveness of local anesthetics [3]. Local anesthetics can have both aminoester or aminoamide structures; most commonly used anesthetics are amides (Table 3. Amides are metabolized within the liver by the cytochrome P450 system, and esters are hydrolyzed by plasma cholinesterases. In sufferers with compromised liver metabolism and in newborns with immature liver operate, amides can produce toxic reactions rather more simply. Local Anesthetic Groups Systemic absorption of injected native anesthetics is dependent upon the positioning of injection and local vascularity. Serum ranges are the highest after intercostal blocks followed by epidurals, caudal blocks, brachial plexus blocks, femoral/sciatic nerve blocks, and subcutaneous injections. Absorption shall be decreased by vasoconstrictors, such as epinephrine, which cut back toxicity, improve analgesia, and extend period of action. Adding epinephrine is simpler with shortacting agents corresponding to lidocaine, which is extended by a minimal of 50%, whereas it has little profit when mixed with bupivacaine for nerve blocks. Addition of sodium bicarbonate raises the pH nearer to the pKa and drives extra extracellular local anesthetic into the non-ionized or base kind. In interventional pain, contrast dye is administered to guarantee correct placement of a needle. Ropivacaine presents additional security over bupivacaine as a result of the right-sided enantiomer, which causes systemic toxicity, is faraway from business ropivacaine (Naropin) but is current in bupivacaine. Sensory fibers are very delicate to local anesthetics and could be blocked with low concentrations of anesthetic with out blocking adjoining motor neurons. Interactions with Local Anesthetics � the motion and unwanted aspect effects of local anesthetics may be considerably influenced by different medicines that the patient is taking for other medical circumstances. Liposomal Bupivacaine Encapsulation of medication into multivesicular liposomes (DepoFoam) offers a novel method to extending drug delivery as multivesicular liposomes have been proven to lead to sustained release lasting over many days to weeks after nonvascular administration. DepoFoam particles are structurally different from unilamellar vesicles, as every comprises a set of closely packed nonconcentric vesicles. Multivesicular liposomes (DepoFoam) are distinctly completely different from unilamellar vesicles and multilamellar vesicles by structure and composition. Unilamellar vesicles have a single bilayer surrounding an aqueous compartment, while multilamellar vesicles have concentric lipid bilayers. DepoFoam particles are composed of nonconcentric a number of lipid layers, which allow for a considerably increased length of action. Practical implications and take-away factors relating to local anesthetics: � Local anesthetics differ extensively in their efficiency and period of action (Table 3. Risks with Local Anesthetic Use � Allergic reactions range from local hypersensitivity to anaphylaxis. Many patients who report allergic reactions are actually delicate to preservatives added to the anesthetic or bisulfites added to epinephrine. Early indicators of toxicity can include irritability, muscle twitching, paresthesias within the arms and periorally, and a metallic taste in the mouth. Severe toxicity could cause convulsive seizures, unconsciousness, and respiratory and cardiovascular depression due to inhibition of central inhibitory tracts. Evidence of lidocaine toxicity may begin at concentrations as little as 5 g/mL (Table 3. Local anesthetics also have a direct vasodilatory effect, which might additional contribute to hypotension. Unconsciousness and convulsions will occur earlier than cardiac toxicity with all local anesthetics besides bupivacaine, which dissociates more slowly from cardiac muscle. Bupivacaine in particular has been shown to have high toxicity in pregnant girls, and concentrated bupivacaine of 0. Corticosteroids Systemic Toxicity Related to Local Anesthetics Management of Local Anesthetic Systemic Toxicity � Toxicity may usually be avoided by means of minimal efficient doses and less poisonous brokers. Edward Calvin Kendall recognized a number of steroid hormones produced in the adrenal cortex in 1935 together with cortisone [13]. Today, glucocorticoids are used for their anti-inflammatory and immune-modulating properties. Half-life in plasma Duration of action (min) (h) 60 90 200 60 one hundred eighty 300 200 200 8�12 8�12 24�36 24�36 24�36 24�36 36�54 36�54 and a lot of different components [14]. The most essential endogenous glucocorticoid is cortisol, which is released in low levels at night time and peaks upon waking. Synthetic glucocorticoids have been created with totally different potencies and durations of action [15] (Table three. Some are available in a depot type, which slowly turns into obtainable over time when injected into the tissue. Chronic corticosteroids can cause an Addisonian crisis when the patient is unable to respond to physiologic stress. Corticosteroids bind to plasma proteins, and decreased proteins mean higher levels of free hormone.