Losartan dosages: 50 mg, 25 mg
Losartan packs: 28 pills, 56 pills, 112 pills, 224 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Trusted 50 mg losartan
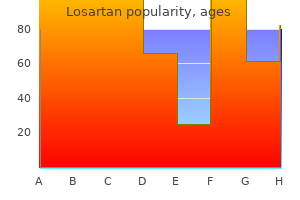
The most vital consequence of renal harm is accumulation of aminoglycosides themselves diabetes while pregnant buy 50mg losartan overnight delivery, which can result in diabetes prevention needs assessment losartan 50mg for sale ototoxicity and even more kidney injury blood glucose 400 purchase losartan 25 mg without a prescription. Most episodes of neuromuscular blockade have occurred following intraperitoneal or intrapleural instillation of aminoglycosides diabetes medications dpp 4 purchase losartan cheap. The threat of paralysis is increased by concurrent use of neuromuscular blocking agents and basic anesthetics. Because of elevated prescriber consciousness, aminoglycoside-induced neuromuscular blockade is now rare. Streptomycin has been associated with neurologic problems (optic nerve dysfunction, peripheral neuritis, paresthesias of the face and hands). Oral neomycin has brought on superinfection of the bowel and intestinal malabsorption. The first sign of impending cochlear injury is high-pitched tinnitus (ringing in the ears). Accordingly, if permanent damage is to be prevented, aminoglycosides must be withdrawn on the first sign of harm (ie, tinnitus, persistent headache, or both). As damage to cochlear hair cells proceeds, listening to within the high-frequency vary begins to decline. Because the initial decline in high-frequency hearing is refined, audiometric testing is required to detect it. The first signal of impending vestibular damage is headache, which can last for 1 or 2 days. Patients should be informed about the symptoms of vestibular and cochlear damage and instructed to report them. These drugs are taken up by tubular cells and obtain excessive intracellular concentrations. Nephrotoxicity correlates with (1) the total cumulative dose of aminoglycosides and (2) high trough levels. Aminoglycoside-induced nephrotoxicity often manifests as acute tubular necrosis. The danger of nephrotoxicity is especially high in older adults, in patients with preexisting kidney illness, and *The trough serum stage is the lowest degree between doses. Penicillins and aminoglycosides are incessantly employed together to improve bacterial kill. The combination is efficient because penicillins disrupt the cell wall, and thereby facilitate entry of aminoglycosides to their site of motion. Unfortunately, when present in high concentrations, penicillins can inactivate aminoglycosides. Like the penicillins, cephalosporins and vancomycin weaken the bacterial cell wall, and may thereby act in concert with aminoglycosides to improve bacterial kill. The threat of injury to the internal ears is considerably increased by concurrent use of ethacrynic acid, a loop diuretic that has ototoxic actions of its personal. Combining aminoglycosides with two different loop diuretics-furosemide and bumetanide-appears to cause no extra ototoxicity than aminoglycosides alone. The risk of renal damage is increased by concurrent remedy with other nephrotoxic brokers. Additive If interstitial fibrosis or renal tubular necrosis develops, damage to the kidneys could also be everlasting. If aminoglycosides are used with these agents, caution have to be exercised to keep away from respiratory arrest. Dosing Schedules Systemic aminoglycosides may be administered as a single large dose each day, or as two or three smaller doses. Traditionally, these drugs have been administered in divided doses, given at equally spaced intervals around-the-clock (eg, each eight hours). Several studies have shown that once-daily doses are simply as effective as divided doses, and possibly safer. Because of this excessive peak focus, and because aminoglycosides exhibit a postantibiotic impact, bacterial kill utilizing a single every day dose is just as great as when we use divided doses-even though, with once-daily dosing, plasma drug levels are subtherapeutic for a chronic time between doses. This prolonged period of low drug ranges additionally explains why once-daily dosing may be very safe: Because levels are low for a really lengthy time, aminoglycosides are capable of wash out from weak cells of the ears and kidneys, thereby reducing harm. In contrast, when we use divided doses, the time throughout which drug ranges are low enough to permit washout is quite short, and hence the risk of toxicity is excessive. To reduce ototoxicity and nephrotoxicity, trough levels have to be sufficiently low. How monitoring is done is dependent upon the dosing schedule employed (ie, once-daily dosing or use of divided doses). For patients receiving divided doses, trough samples should be taken just earlier than the subsequent dose. For sufferers receiving once-daily doses, a single pattern can be drawn 1 hour before the next dose. Unfortunately, resistance to gentamicin is rising, and crossresistance to tobramycin is widespread. For infections which may be immune to gentamicin and tobramycin, amikacin is usually effective. In addition to its use in opposition to gram-negative bacilli, gentamicin can be mixed with vancomycin, a cephalosporin, or a penicillin to treat serious infections brought on by certain grampositive cocci, specifically, Enterococcus species, some streptococci, and Staph. The curves depict plasma levels of gentamicin produced with (1) a single large dose administered as soon as a day versus (2) the identical daily complete given as three smaller doses spaced eight hours apart. Plasma ranges with each regimens are high enough to produce good bactericidal effects. The shaded area signifies levels that are low sufficient to allow washout of the drug from susceptible cells in the inner ears. Note that, with oncedaily dosing, levels are within the washout vary for over 12 hours, versus a complete of only 6 hours when divided doses are used. As a result, ototoxicity and nephrotoxicity are lower with the once-a-day schedule. Caution have to be exercised when combining gentamicin with different nephrotoxic or ototoxic drugs. Preparations, Dosage, and Administration Treatment of Gram-Negative Infections Intravenous and Intramuscular. For adults, the normal dosing scheme consists of a loading dose (2 mg/kg) adopted by doses of 1 to 1. When once-daily dosing is employed, the dosage is 5 mg/kg every 24 hours; no loading dose is required. In adults and children with renal impairment, the entire every day dosage should be reduced. Peak levels ought to range between 4 and 10 mcg/mL (for conventional dosing) or between sixteen and 24 mcg/mL (for once-daily dosing). For all patients, therapy should continue for 1 day after samples of cerebrospinal fluid turn out to be unfavorable for the infecting organism. As noted, gentamicin could also be combined with vancomycin, a penicillin, or a cephalosporin to deal with critical infections caused by Enterococcus species, certain streptococci, and Staph. When gentamicin is used on this way, dosages are a lot decrease than when the drug is used in opposition to gram-negative infections. For mixture remedy, a typical dosage for adults is 1 mg/kg/day, compared with three to 5 mg/ kg/day when the drug is utilized by itself. Amikacin has two outstanding options: (1) of all of the aminoglycosides, amikacin is energetic in opposition to the broadest spectrum of gram-negative bacilli and (2) of all the aminoglycosides, amikacin is the least vulnerable to inactivation by bacterial enzymes. In hospitals the place resistance to gentamicin and tobramycin is common, amikacin is the preferred agent for initial remedy of infections attributable to cardio gram-negative bacilli. However, in settings the place resistance to the other aminoglycosides is infrequent, amikacin should be reserved for infections of proven aminoglycoside resistance because this apply will delay emergence of organisms proof against amikacin. Caution must be exercised if amikacin is utilized in mixture with different ototoxic or nephrotoxic medication. The really helpful dosage for adults and children is 15 mg/kg/day administered both (1) as a single day by day dose or (2) in equally divided doses given 8 or 12 hours aside.
Purchase genuine losartan on-line
Preferred brokers for prophylaxis of disseminated infection are azithromycin and clarithromycin diabetes for dummies purchase 25mg losartan overnight delivery. Regimens for treating energetic an infection in immunocompetent hosts ought to embody (1) azithromycin or clarithromycin plus (2) ethambutol plus (3) rifampin or rifabutin diabetes symptoms hyperglycemia order 50mg losartan overnight delivery. Additional medicine may be added as wanted; options embrace streptomycin diabetes diet without medication losartan 25 mg generic, ciprofloxacin diabetes diet pdf spanish order on line losartan, and amikacin. Treatment of lively an infection in immunocompetent patients ought to continue for 12 months after cultures turn out to be negative. Dapsone is chemically associated to the sulfonamides and shares their mechanism of action: inhibition of folic acid synthesis. Accordingly, isolates from all patients must bear testing of drug sensitivity, a process that sometimes takes several weeks. Patient adherence could be tremendously increased by utilizing directly noticed remedy mixed with intermittent, rather than every day, dosing. Accordingly, when these three medication are mixed, as they usually are, the risk of liver injury may be substantial. However, a much easier regimen-isoniazid plus rifapentine taken as soon as per week for just three months-is just as effective and is likely to replace isoniazid alone as commonplace remedy. Inform sufferers about signs of hepatitis (jaundice, anorexia, malaise, fatigue, nausea), and instruct them to notify the prescriber immediately if these develop. To promote adherence, educate the patient about the rationale for multidrug therapy and the necessity for long-term treatment. Encourage patients to take their medicine precisely as prescribed, and to continue treatment until the an infection has resolved. In patients at high danger of neuropathy (eg, alcohol abusers, diabetic patients), give pyridoxine prophylactically. Isoniazid can suppress the metabolism of phenytoin, thereby causing phenytoin levels to rise. Inform sufferers about symptoms of peripheral neuropathy (tingling, numbness, burning, or pain within the hands or feet), and instruct them to notify the prescriber if these occur. Preadministration Assessment Therapeutic Goal Treatment of energetic or latent tuberculosis. Baseline Data Obtain a chest radiograph, microbiologic exams of sputum, and baseline checks of liver operate. Use with warning in alcohol abusers, sufferers with liver illness, and patients taking warfarin. Administration Instruct the affected person to take oral rifampin as soon as a day, either 1 hour before a meal or 2 hours after. Identifying High-Risk Patients Isoniazid is contraindicated for patients with acute liver illness or a historical past of isoniazid-induced hepatotoxicity. Administration Advise sufferers to take isoniazid on an empty stomach, both 1 hour before meals or 2 hours after. Inform sufferers about indicators of liver dysfunction Administration Usually administered as soon as a day. Inform patients about symptoms of hepatitis (malaise, anorexia, nausea, vomiting, yellowish discoloration of the skin and eyes), and instruct them to notify the prescriber if these develop. Inform sufferers that rifampin might impart a harmless red-orange colour to urine, sweat, saliva, and tears. Warn sufferers that delicate contact lenses may endure everlasting staining; advise them to consult an ophthalmologist about continued use of the lenses. Tests of liver operate must be made before therapy and each 2 to 4 weeks thereafter. The threat of liver injury is increased by concurrent remedy with isoniazid, rifampin, rifabutin, or rifapentine, all of which are hepatotoxic. Minimizing Adverse Interactions can speed up the metabolism of many medication, thereby lowering their results. Advise ladies taking oral contraceptives to use a nonhormonal type of contraception. Baseline Data Obtain a chest radiograph, microbiologic exams of sputum, and baseline vision tests. Identifying High-Risk Patients Ethambutol is contraindicated for sufferers with optic neuritis. Advise patients to take Ongoing Evaluation and Interventions Minimizing Adverse Effects Optic Neuritis. Symptoms include blurred imaginative and prescient, altered color discrimination, and constriction of visible fields. Identifying High-Risk Patients Pyrazinamide is contraindicated for sufferers with severe liver dysfunction or acute gout. Oral ciprofloxacin has been used as an alternative to parenteral antibiotics for treatment of a number of severe infections. However, unlike nalidixic acid, the fluoroquinolones are broad-spectrum agents that have a quantity of purposes. As a result, these drugs are attractive options for people who may in any other case require intravenous antibacterial therapy. Although side effects are typically mild, all fluoroquinolones can cause tendinitis and tendon rupture, normally of the Achilles tendon. Bacterial resistance develops slowly, however has turn into frequent in Neisseria gonorrhoeae, and hence these medicine are no longer recommended for this infection. Fluoroquinolones used solely for topical remedy of the eyes are discussed in Chapter 104. Antimicrobial Spectrum Ciprofloxacin is active in opposition to a broad spectrum of micro organism, including most cardio gram-negative bacteria and some gram-positive micro organism. Most urinary tract pathogens, including Escherichia coli and Klebsiella, are delicate. The drug is also extremely energetic in opposition to most micro organism that cause enteritis (eg, Salmonella, Shigella, Campylobacter jejuni, E. Other delicate organisms embody Bacillus anthracis, Pseudomonas aeruginosa, Haemophilus influenzae, meningococci, and many streptococci. Ciprofloxacin Ciprofloxacin [Cipro] was among the first fluoroquinolones available and can serve as our prototype for the group. The drug is lively towards a broad spectrum of bacterial pathogens, Bacterial Resistance Resistance to fluoroquinolones has developed during remedy of infections attributable to Staphylococcus aureus, Serratia marcescens, C. High concentrations are achieved in urine, stool, bile, saliva, bone, and prostate tissue. Also, ciprofloxacin is a most popular drug for preventing anthrax in individuals who have inhaled anthrax spores. Because ciprofloxacin is energetic towards quite lots of pathogens and can be given orally, the drug represents an various to parenteral remedy for many critical infections. Owing to high rates of resistance, ciprofloxacin is a poor alternative for staphylococcal infections. Because of issues about tendon injury (see below), systemic ciprofloxacin is mostly prevented in youngsters beneath 18 years old. Nonetheless, the drug does have two approved pediatric makes use of: (1) remedy of difficult urinary tract and kidney infections brought on by E. In older adults, ciprofloxacin poses a big threat of confusion, somnolence, psychosis, and visual disturbances. Rarely, ciprofloxacin and other fluoroquinolones have caused tendon rupture, normally of the Achilles tendon. People at highest threat are these 60 and older, those taking glucocorticoids, and those who have undergone coronary heart, lung, or kidney transplantation. Fluoroquinolones injury tendons by disrupting the extracellular matrix of cartilage in immature animals. Since tendon damage is reversible if diagnosed early, fluoroquinolones should be discontinued at the first sign of tendon pain, swelling, or inflammation. In addition, patients should chorus from exercise till tendinitis has been dominated out.
Diseases
- Facio digito genital syndrome recessive form
- Lymphangiomyomatosis
- Giedion syndrome
- Apiphobia
- Schaap Taylor Baraitser syndrome
- Ballard syndrome
- Pie Torcido
- X chromosome, trisomy Xp3
Cheapest losartan
Abiraterone is equipped in 250-mg capsules diabetes symptoms early pregnancy purchase generic losartan from india, which must be swallowed with water on an empty abdomen (1 hour before a meal or 2 hours after) diabete 66 cheap losartan online. The usual regimen is one thousand mg abiraterone once day by day combined with 5 mg prednisone twice day by day diabetic diet urdu effective losartan 25 mg. Ketoconazole Ketoconazole [Nizoral] diabetes type 1 meaning cheap losartan 25 mg without a prescription, used primarily for fungal infections (see Chapter 92), can be used off-label for prostate cancer. As with abiraterone, advantages derive from inhibiting testicular, adrenal, and prostatic production of androgens. Dosages are larger than those used for antifungal therapy (400 mg three instances a day in contrast with 200 mg as soon as a day), and therefore unwanted effects are frequent. Among these are nausea, vomiting, fatigue, skin adjustments, liver damage, and gynecomastia. Because high-dose ketoconazole can suppress adrenal production of glucocorticoids, the drug is normally mixed with hydrocortisone (to keep away from adrenal insufficiency). Nonetheless, sipuleucel-This of great interest in that it represents an entirely new method to cancer therapy. Sipuleucel-This indicated for therapy of asymptomatic or minimally symptomatic metastatic castration-resistant (hormone-refractory) prostate most cancers. In clinical trials, sipuleucel-T prolonged life by about four months, in contrast with 2. Sipuleucel-This produced in two steps: collection of circulating immune cells (macrophages) from the patient, adopted by modification of those cells in the laboratory. This process-cell collection plus modification-takes about 2 days, and must be done for every dose. Macrophage collection is done by leukapheresis, a course of by which venous blood is circulated from the patient, via a machine, after which again into the affected person. The machine separates out macrophages (along with some platelets and different blood cells), and then returns the remaining cells and serum to the patient. The commonest are chills, fatigue, fever, back ache, nausea, joint ache, and headache. Other widespread reactions embody paresthesias, vomiting, anemia, constipation, dizziness, weak spot, and extremity pain. Symptoms embrace fever, chills, nausea, vomiting, fatigue, hypertension, tachycardia, and respiratory reactions (dyspnea, hypoxia, and bronchospasm). Infusion reactions could be decreased by premedication with acetaminophen plus an antihistamine, similar to diphenhydramine [Benadryl]. Pretreatment with acetaminophen plus an antihistamine can scale back infusion reactions. Either drug (in mixture with prednisone) can prolong total survival as well as progression-free survival. At this time, docetaxel is taken into account a first-line drug for hormone-refractory prostate most cancers. The major antagonistic effects of docetaxel are neutropenia, hypersensitivity reactions, and fluid retention. The major adverse results of cabazitaxel are neutropenia, hypersensitivity reactions, anemia, and diarrhea. Estramustine Estramustine [Emcyt] is a hybrid molecule composed of estradiol (an estrogen) coupled to nitrogen mustard (an alkylating agent; see Chapter 102). The only indication for the drug is palliative therapy of superior prostate most cancers. Estramustine is run orally, and becomes concentrated in prostate cells, apparently via the actions of a singular "estramustine-binding protein. Third, and most importantly, the drug binds to microtubules of mitotic spindles, and thereby disrupts mitosis. The most severe effect is thrombosis, with resultant myocardial infarction and stroke. Other opposed results include fluid retention, nausea, vomiting, diarrhea, and hypercalcemia. The hope is that these drugs shall be extra selective than hormones and cytotoxic anticancer medicine, and therefore will be succesful of destroy most cancers cells whereas leaving regular cells untouched. A few focused drugs, such as imatinib [Gleevec], have been remarkably profitable, producing full responses with relatively delicate adverse results. Unfortunately, with many different focused medicine, responses have been less spectacular, whereas opposed results have been more extreme. Nonetheless, the concept of focused therapy has nice attraction, and intensive analysis is underway to make it extra of a actuality. Many of these medicine are antibodies that bind with particular antigens on tumor cells; others are small molecules that inhibit intracellular enzymes. Some antibodies mark most cancers cells for immune attack, some block cell-surface receptors, some ship toxic medication or radioactivity, and some inhibit angiogenesis, and thereby deprive tumor cells of their blood provide. Most of the small molecules inhibit particular tyrosine kinases, and thereby disrupt intracellular signaling pathways. The different 4 drugs-erlotinib, gefitinib, afatinib, and lapatinib-are small molecules that work inside the cell to inhibit tyrosine kinase directly. This process, often identified as phosphorylation, alters the construction of the acceptor protein, and thereby increases or decreases its activity. Put another method, the outcomes of phosphorylation is like flipping a swap, turning it on or turning it off. For example, certain regulatory proteins, when phosphorylated, activate signaling pathways that improve cell proliferation and cell survival. Accordingly, if we stop phosphorylation with a kinase inhibitor, we are in a position to shut down the signaling pathway, and thereby inhibit proliferation and promote apoptosis (programmed cell death). The drug is permitted for refractory colorectal cancer and for carcinoma of the pinnacle and neck. As noted, these receptors, which assist regulate cell progress, are overexpressed in sure cancers, together with these of the colon and rectum. Cetuximab, in combination with radiation, is approved for initial therapy of locally or regionally advanced squamous cell carcinoma of the top and neck. In addition, the drug can be utilized for recurrent or metastatic cancers that have progressed regardless of treatment with a platinum-based regimen. Manifestations embrace rapid-onset airway obstruction, hypotension, shock, lack of consciousness, myocardial infarction, and cardiopulmonary arrest. Severe reactions can occur with any infusion, however most (90%) happen with the first infusion. If a severe reaction develops, cetuximab must be discontinued instantly and never used again. Ocular effects- amblyopia, conjunctivitis, eye ache, and corneal erosion or ulceration-occur sometimes. If respiratory signs develop, gefitinib ought to be interrupted and the patient evaluated. Likewise, medication that decrease gastric pH (eg, histamine2 antagonists, proton pump inhibitors, antacids) can lower gefitinib absorption, and should thereby decrease its level. In laboratory animals, the drug decreased the variety of reside births, elevated neonatal mortality, and lowered fetal weight. Acne-like rash, mainly on the face and higher torso, develops in 88% of sufferers, and is severe in 12%. Severe rash has led to Staphylococcus aureus sepsis and abscesses that require incision and drainage. Sunlight can exacerbate dermatologic reactions, and hence sufferers ought to limit solar publicity, use a sunblock, and wear protecting clothes. Very hardly ever, cetuximab has been related to interstitial lung disease, characterised by inflammation, scarring, and hardening of the lungs. One case of deadly interstitial pneumonitis with pulmonary edema has been reported. Whether cetuximab is really the cause for these lung issues has not been established. In medical trials, hypomagnesemia developed in 55% of sufferers, and was extreme in 6% to 17%.
Generic losartan 25 mg online
There are smaller contributions from branches of the lingual diabete mellitus type 1 losartan 25 mg lowest price, the ascending pharyngeal and the ascending palatine arteries blood glucose goals for gestational diabetes proven 25 mg losartan. The venous drainage is by way of a venous plexus that pierces the superior constrictor muscle diabetes type 2 zenuwpijn order losartan 50 mg mastercard. At the hamulus the superior constrictor attachment continues inferiorly alongside the pterygomandibular raphe to the mandible on the posterior finish of the mylohyoid line stage with the border of the last molar diabetes prevention flyer discount losartan 25 mg without prescription. Attachment to this raphe is shared by the buccinator muscle, which extends anteriorly, while the superior constrictor extends posteriorly. As with the other constrictor muscles, the fibres of the superior constrictor extend around the pharynx to join within the midline on the pharyngeal raphe. Most of the superior constrictor fibres lengthen upwards, but the muscle is present as low as the extent of the vocal cords inside the center constrictor muscle. At either facet of the epiglottis the lateral glossoepiglottic folds separate it from the oropharynx. Below these folds lie the piriform fossae, which sit lateral to the quadrangular cartilage of the larynx and medial to the interior floor of the thyroid cartilage inferiorly and the thyrohyoid membrane superiorly. The stiffness of this fascia maintains the patency of the nasopharynx during breathing. In the midline posteriorly running the length of the pharynx is the pharyngeal raphe. This receives fibres from all of the constrictor muscular tissues and attaches to the pharyngeal tubercle on the clivus. The attachment of the pharygobasilar fascia then passes laterally and anteriorly over the foramen lacerum to just in front of the carotid canal. It then leaves its bony attachment and is connected to the cartilaginous portion of the auditory tube earlier than attaching to the posterior border of the medial pterygoid plate to the hamulus. As this ligament attaches to the lesser cornu of the hyoid bone, the middle constrictor attachment extends along the superior surface of the higher cornu of the hyoid bone. The fibres again prolong posteriorly to meet at the pharyngeal raphe, diverging extensively. The uppermost fibres of the middle constrictor can completely enclose the superior constrictor muscle, and inferiorly fibres once more prolong as far as the vocal cords. The area between the superior and middle constrictor muscle tissue is filled by the tongue base. Passing by way of this space are the structures that cross from outside the pharynx to the oral cavity, the stylopharyngeus muscle and the glossopharyngeal and lingual nerves. The thyropharyngeus arises from the oblique line on the thyroid lamina and inferior to this from a fibrous arch overlying the cricorthyroid muscle, ending at the inferior border of the cricoid cartilage. Its fibres diverge broadly as it passes backwards enclosing the middle and superior constrictor muscular tissues to the pharyngeal raphe. The thyropharyngeus fibres extend superiorly nearly to the level of the pharyngeal tubercle. The inferior fibres journey horizontally with the superior fringe of the cricopharyngeus muscle. The hole between the center constrictor muscle and the thyropharyngeus muscle is closed by the thyrohyoid membrane. Passing via this hole are the inner department of the superior laryngeal nerve and the superior laryngeal vessels. Whilst the opposite constrictor muscle tissue are flat sheets of muscle, the cricopharyngeus muscle is rounder and thicker and extends fully around the pharynx without becoming a member of the pharyngeal raphe. It is in continuity inferiorly with the round muscular layer of the oesophagus and acts as a sphincter between the lowest extent of the pharynx and the upper oesophagus. This sphincter stays closed except during swallowing, which prevents air from being sucked into the oesophagus throughout inhalation. The cricopharyngeus muscle may be supplied by the recurrent laryngeal nerve or the exterior laryngeal nerve immediately rather than from the pharyngeal plexus. The soft palate is made up of an aponeurosis, which is acted on by five paired muscle tissue. The tensor palati is a triangular muscle attaching to the scaphoid fossa on the medial pterygoid plate, the lateral edge of the auditory tube and the spine of the sphenoid. From this broad insertion the muscle comes together as a tendon on the pterygoid hamulus, where it turns at a proper angle and enters the pharynx. The tendon now broadens out, forming the aponeurosis of the taste bud connected anteriorly to the crest of the palatine bone and mixing within the midline. The aponeurosis is concave in the course of the mouth so that when the tensor palati contracts, the taste bud is flattened inferiorly. Because this muscle attaches to the auditory tube, contraction also pulls on this structure, opening it and permitting equalization of pressure between the nasopharynx and the center ear. The levator palati muscle is a round muscle arising at the quadrate area of the petrous bone and the adjacent medial side of the cartilaginous auditory tube. It inserts onto the nasal floor of the aponeurosis between the 2 heads of the palatopharyngeus. Contraction of this muscle pulls the taste bud upwards and posteriorly and again opens the auditory tube. The palatoglossus arises from the inferior floor of the aponeurosis and passes downwards to interdigitate with the styloglossus. This muscle varieties the anterior tonsillar pillar and delineates the junction between the oral cavity and the oropharynx. The palatopharyngeus arises from two heads, one hooked up to the onerous palate and one on the aponeurosis on either aspect of the levator palati muscle. The two heads fuse and head inferiorly, forming the posterior pillar of the tonsil, and insert into the posterior border of the thyroid lamina passing deep to the constrictors. The stylopharyngeus muscle arises from the styloid process and inserts into the posterior border of the thyroid lamina. This muscle is supplied by the glossopharyngeal nerve immediately and not the pharyngeal plexus. Venous drainage is into the venous pharyngeal plexus at the back of the center constrictor, which drains into the pterygoid plexus and the internal jugular vein. The motor supply of the pharynx is from the pharyngeal plexus mendacity on the posterolateral wall of the pharynx and is made up by branches of the vagus and glossopharyngeal nerves and the cervical sympathetic trunk. Sensory supply of the nasopharynx is from the pharyngeal branch of the maxillary nerve, and the sensory supply of the oropharynx is from the glossopharyngeal nerve apart from the vallecula, which is equipped by the internal department of the superior laryngeal nerve. The remainder of the pharyngeal mucosa is equipped by the interior branch of the superior laryngeal nerve and the recurrent laryngeal nerve. The challenge is to distinguish between these with benign disease and people with critical conditions with out overinvestigating the former. Frequently, this might be as a outcome of viral pharyngitis or tonsillitis, however unilateral signs should alert one to focal and probably more severe disease. Persistence past a period that might be anticipated for widespread infections also warrants attention/ concern (4 weeks is a sensible time point). Pain originating from the tonsil will be made worse by swallowing and may be referred to the ear because the glossopharyngeal nerve provides both websites. Persistent pain and trismus counsel either quinsy or unfold of an oropharyngeal tumour to the pterygoid muscles. There could additionally be an incapability to swallow sure foodstuffs, for instance lumps of meat. This may be an early symptom of cancer but is more commonly as a end result of different things, including cricopharyngeal spasm, oesophageal dysmotility, pharyngeal pouch, laryngopharyngeal reflux and exterior compression from a thyroid goitre or globus pharyngeus. Painful swallowing (odynophagia) is most commonly attributable to tonsillar infections however can be a symptom of cancers of the pharynx. Regurgitation, especially of recently eaten but undigested food, suggests a pharyngeal pouch. Furthermore, invasion of the cranium base by a nasopharyngeal tumour may find yourself in cranial nerve palsies presenting as diplopia, facial ache, uncoordinated swallowing, hypernasality from a paralyzed palate and dysphonia from a paralyzed vocal fold. Conductive hearing loss may result from glue ear secondary to nasopharyngeal illness. However, within the very sensitive patient or the affected person with a congested nostril, topical decongestant and local anaesthesia must be used.
Best buy losartan
Like other nucleoside analogs diabetes symptoms dizziness losartan 25 mg visa, emtricitabine might pose a risk of lactic acidosis and severe hepatomegaly with steatosis diabete tipo 01 buy generic losartan pills, usually in ladies diabetes insipidus diagnosis order losartan 25mg without a prescription. Combination Products the availability of combination antiretroviral products has simplified remedy diabetes insipidus zentral renal generic 50mg losartan with mastercard. In truth, with two combination products-Atripla and Complera- patients can now be treated with one tablet as soon as a day. As anticipated, each drug in the mixture brings with it the opposed reactions and drug interactions inherent in that drug. Nucleotides and nucleosides are very similar (a nucleotide is solely a nucleoside with a phosphate group added) and hence have related effects on reverse transcriptase. The drug is effective and, due to its lengthy half-life, may be administered as soon as a day. Administration with a high-fat meal can enhance plasma levels by 39% (using efavirenz capsules) and by 50% (using efavirenz tablets). The drug has a long serum half-life (40 to fifty five hours), and hence can be taken just once a day. Efavirenz can compete with other medicine for metabolism by cytochrome P450, thereby inflicting them to accumulate, presumably to harmful ranges. Efavirenz induces P450, and may thereby accelerate its personal metabolism and the metabolism of many other medicine. Increased metabolism of two protease inhibitors-saquinavir and indinavir-is of specific concern. If efavirenz is combined with indinavir, the dosage of indinavir must be elevated. By inducing P450, efavirenz can decrease the consequences of hormonal contraceptives, including oral contraceptives and the etonogestrel contraceptive implant. Combining efavirenz with ritonavir (a protease inhibitor that inhibits P450) can enhance levels of each medicine. The principal mechanism is accelerated metabolism secondary to induction of P450 (see Chapter 108). Efavirenz [Sustiva] is on the market in 600-mg tablets and in capsules (50 and 200 mg). The most typical are dizziness, insomnia, impaired consciousness, drowsiness, vivid desires, and nightmares. Delusions, hallucinations, and extreme acute despair may also happen, primarily in sufferers with a history of mental illness or drug abuse. Rash can range in severity from delicate (erythema, pruritus) to moderate (diffuse maculopapular rash, dry desquamation) to severe (vesiculation, moist desquamation, ulceration). Very not often, rash evolves into potentially fatal Stevens-Johnson syndrome, erythema multiforme, or poisonous epidermal necrolysis. In monkeys, doses equivalent to these utilized in humans produced a high incidence of fetal malformation. A barrier technique of contraception (eg, condom) should be used along side a hormonal technique (eg, oral contraceptive). Selected content material (pharmacokinetics, preparations, dosage, administration, drug interactions, and some adverse effects) is out there in Table 94�4 for the remaining medication. Accordingly, nevirapine ought to always be combined with other antiretroviral drugs. The commonest adverse impact is rash, which normally happens early in therapy and can be extreme and even life threatening. For most patients, the rash is benign and, if wanted, may be managed with an antihistamine or topical glucocorticoid. However, if the affected person experiences extreme rash or rash related to fever, blistering, oral lesions, conjunctivitis, muscle ache, or joint ache, nevirapine must be withdrawn. Because these signs might point out development of erythema multiforme or Stevens-Johnson syndrome. Nevirapine can cause severe hepatotoxicity, together with fulminant and cholestatic hepatitis, hepatic necrosis, and hepatic failure. The risk is highest during the first 12 weeks of treatment, and is elevated by a history of chronic hepatitis B or hepatitis C. Liver perform checks must be accomplished at baseline, before dosage escalation, 2 weeks after dosage escalation, and each time patients have signs (fatigue, malaise, anorexia, nausea) suggesting an early stage of liver injury. If hepatotoxicity is diagnosed, nevirapine ought to be withdrawn as soon as potential. High-fat meals enhance plasma ranges by 39% with capsules and by 79% with tablets. Always use a drug interaction checker (software utility or online) to confirm security before administering non-nucleoside reverse transcriptase inhibitors with different drugs. Nevirapine is both an inducer and substrate of cytochrome P450, and can thereby increase the metabolism of other drugs, inflicting their ranges to decline. The ability to decrease ranges of protease inhibitors, hormonal contraceptives, and methadone is of specific concern. However, widespread use of those medication has revealed additional unwanted effects: fat redistribution, hyperglycemia and diabetes, reduced bone mineral density, increased bleeding in hemophiliacs, and elevation of triglyceride and transaminase levels. Additionally, all of them act as both inhibitors of some isoenzymes and inducers of others. Sometimes they may even act each as inhibitors and inducers of the identical isoenzymes. Accordingly, until such information become out there, choice amongst them must be primarily based on different components, primarily facet effect profile, drug interactions, and patient acceptance. Like efavirenz, delavirdine causes potentially severe rash and different hypersensitivity reactions. In scientific trials, rash developed in up to 50% of patients; erythema multiforme and Stevens-Johnson syndrome have been reported not often. In distinction to efavirenz and nevirapine, which induce cytochrome P450, delavirdine inhibits cytochrome P450. In scientific trials, gentle to moderate rash developed in up to 9% of sufferers, but the incidence of severe skin reactions-StevensJohnson syndrome, toxic epidermal necrolysis, erythema multiforme-was low: less than 1%. Etravirine ought to be discontinued immediately if a severe hypersensitivity reaction develops. Signs and signs embrace severe rash, or rash accompanied by fever, malaise, fatigue, blisters, oral lesions, conjunctivitis, facial edema, hepatitis, muscle aches, or joint aches. Compared with efavirenz, rilpivirine is simply as effective and presumably better tolerated-but carries a higher danger of resistance and virologic failure, especially in sufferers with a high viral load (>100,000 virions/mL). Three major mechanisms are concerned: inhibition of P450, induction of P450, and elevation of gastric pH. Protease inhibitors have been related to hyperglycemia, new-onset diabetes, abrupt exacerbation of present diabetes, and diabetic ketoacidosis. Onset typically happens after 2 months of drug use, however can even develop a lot earlier. Hyperglycemia may be managed with insulin and oral antidiabetic brokers (eg, metformin). Because of the potential risk of diabetes, patients must be instructed to report indicators of the illness, similar to polydipsia (increased fluid intake), polyphagia (increased food intake), and polyuria (frequent urination). Fat accumulates within the abdomen ("protease paunch"), within the breasts of men and women, and between the shoulder blades ("buffalo hump"). Health risks of the syndrome are unknown, though it can be psychologically distressing. Sculptra is an injectable type of poly-L-lactic acid, a biodegradable artificial polymer that has been widely utilized in dissolvable stitches, bone screws, and facial implants. Administration is by direct injection into the deep dermis or subcutaneous tissue using a 26-gauge needle. After the preliminary sequence of injections, repeat therapies could additionally be wanted to maintain the correction. Principal adverse effects are native reactions, including redness, swelling, bruising, and growth of nodules. In clinical trials, tesamorelin decreased visceral abdominal adipose tissue by 14% to 18%-about the identical reduction that might be achieved with food regimen and train.
Syndromes
- Does the person have epilepsy or a seizure disorder?
- Rapidly worsening symptoms of alkalosis
- Medications such as birth control pills, diet pills, some cold medicines, and migraine medicines
- Are you vomiting undigested food?
- Treat the sore as directed by your doctor or nurse.
- How ability to function has changed
- Diverticula
Losartan 50 mg overnight delivery
In sufferers with renal impairment diabetes medications depression purchase 25mg losartan, as indicated by decreased creatinine clearance diabetes mellitus versi indonesia buy losartan 25 mg visa, dosage must be decreased blood sugar 3 hours after eating 50mg losartan amex. Aztreonam [Azactam diabetes mellitus simple definition buy losartan 50mg without prescription, Cayston] belongs to a class of betalactam antibiotics generally recognized as monobactams. Therefore, like most beta-lactam antibiotics, the drug inhibits bacterial cell wall synthesis, and thereby promotes cell lysis and dying. Aztreonam has a slim antimicrobial spectrum, being lively solely towards gram-negative cardio bacteria. Aztreonam is extremely resistant to beta-lactamases, and therefore is energetic against many gram-negative aerobes that produce them. Hence, aztreonam appears protected for patients with allergic reactions to other beta-lactam antibiotics. Aztreonam is on the market in powdered type, sold as Cayston, to be reconstituted with the diluent provided, after which inhaled using the Altera Nebulizer System. Dosing is finished as a repeating cycle of 75 mg 3 occasions a day for 28 days, adopted by 28 days off. Telavancin [Vibativ] is the first consultant of a new class of agents, the lipoglycoproteins, artificial derivatives of vancomycin. Second, telavancin binds to the bacterial cell membrane and thereby disrupts membrane function. In patients with renal impairment, the half-life is extended and blood ranges improve. In sufferers with moderate hepatic impairment, the kinetics of telavancin stay unchanged. As with vancomycin, fast infusion can cause "pink man syndrome," characterized by flushing, rash, pruritus, urticaria, tachycardia, and hypotension. Fosfomycin may also cause belly pain, rhinitis, drowsiness, dizziness, and rash. Fosfomycin Fosfomycin [Monurol] is a singular antibiotic approved for single-dose therapy in ladies with uncomplicated urinary tract infections (ie, acute cystitis) caused by E. The drug kills micro organism by disrupting synthesis of the peptidoglycan polymer strands that compose the cell wall. Except for ceftriaxone, all cephalosporins are eliminated by the kidneys, and subsequently must be given in lowered dosage to sufferers with renal impairment. Patients allergic to penicillins have a few 1% threat of cross-reactivity with cephalosporins. Two cephalosporins-cefazolin and cefotetan-can cause a disulfiram-like response. Preadministration Assessment Therapeutic Goal Treatment of infections attributable to vulnerable organisms. Baseline Data the prescriber could order tests to determine the identity and drug sensitivity of the infecting organism. Identifying High-Risk Patients Cephalosporins are contraindicated for sufferers with a history of allergic reactions to cephalosporins or of severe allergic reactions to penicillins. Dosages for all cephalosporins-except ceftriaxone-should be reduced in patients with important renal impairment. Check the injection web site for induration, tenderness, and redness-and notify the prescriber if these happen. Cefditoren is excreted in combination with carnitine, and might thereby lower carnitine levels. Do not give cefditoren to sufferers with preexisting carnitine deficiency or with conditions that predispose to carnitine deficiency. In patients aside from neonates, ceftriaxone and calcium-containing solutions could additionally be administered sequentially, supplied the infusion line is flushed between infusions. Ongoing Evaluation and Interventions Evaluating Therapeutic Effects Monitor for indications of antimicrobial effects (eg, discount in fever, pain, or inflammation; improved appetite or sense of well-being). Avoid cephalosporins in patients with a historical past of cephalosporin allergy or extreme penicillin allergy. Instruct the patient to report any signs of allergy (eg, skin rash, itching, hives). If anaphylaxis occurs, administer parenteral epinephrine and provide respiratory assist. Observe sufferers for indicators of bleeding and, if bleeding develops, discontinue the drug. To decrease this response, rotate the injection web site and inject cephalosporins slowly and in dilute resolution. Observe the affected person for phlebitis and alter the infusion website if phlebitis develops. Treat with metronidazole or vancomycin, relying on the severity of the an infection. Baseline Data the prescriber could order tests to determine the identity and drug sensitivity of the infecting organisms. Identifying High Risk Patients Exercise caution in patients with renal impairment. Adjust the dosage to obtain an efficient trough serum degree: 15 to 20 mcg/mL for critical infections and 10 mcg/mL for less critical infections. Instruct sufferers to full the prescribed course of remedy despite the fact that signs could abate earlier than the full course is over. If significant kidney harm develops, as indicated by a 50% enhance in serum creatinine level, dosage ought to be decreased. Rapid infusion may cause "purple man syndrome," characterised by flushing, rash, pruritus, urticaria, tachycardia, and hypotension. To assist keep away from this widespread reaction, use vancomycin in dilute solution and alter the infusion web site typically. Ongoing Evaluation and Interventions Evaluating Therapeutic Effects Monitor for indications of antimicrobial results (eg, discount in fever, ache, or inflammation; improved urge for food or *Patient schooling info is highlighted as blue textual content. Selective toxicity of the tetracyclines results from their poor capacity to cross mammalian cell membranes. To affect protein synthesis, tetracyclines must first acquire entry to the cell inside. Consequently, although tetracyclines are inherently capable of inhibiting protein synthesis in mammalian cells, their levels within host cells stay too low to be harmful. Microbial Resistance Bacterial resistance results from increased drug inactivation, decreased access to ribosomes (owing to the presence of ribosome safety proteins), and decreased intracellular accumulation (owing to decreased uptake and elevated export). Sensitive organisms embrace Rickettsia, spirochetes, Brucella, Chlamydia, Mycoplasma, Helicobacter pylori, Borrelia burgdorferi, Bacillus anthracis, and Vibrio cholerae. However, unlike the aminoglycosides, which are bactericidal, the medication thought-about listed here are largely bacteriostatic. In common, the drugs introduced listed here are second-line agents, used primarily for infections resistant to first-line brokers. Because of resistance, and since antibiotics with higher selectivity and fewer toxicity are now out there, use of tetracyclines has declined. Beneficial results derive from suppressing the growth and metabolic activity of Propionibacterium acnes, an organism that secretes inflammatory chemicals. Helicobacter pylori, a bacterium that lives within the abdomen, is a major contributing factor to peptic ulcer disease. All four-tetracycline, demeclocycline, doxycycline, and minocycline-are related in construction, antimicrobial actions, and opposed results. Mechanism of Action the tetracyclines suppress bacterial development by inhibiting protein synthesis. Doxycycline is used orally and topically, whereas minocycline is used solely topically. Benefits of oral doxycycline [Periostat] result from inhibiting collagenase, an enzyme that destroys connective tissue within the gums. Topical minocycline [Arestin] and doxycycline [Atridox] are employed as adjuncts to scaling and root planing. The objective is to scale back pocket depth and bleeding in adults with periodontitis. Minocycline can scale back symptoms in patients with rheumatoid arthritis, suggesting a potential infectious element to the disease. Ultimate elimination of short- and intermediate-acting tetracyclines-tetracycline and demeclocycline-is in the urine, largely as the unchanged drug.
Buy genuine losartan on-line
To minimize danger diabetes gene test buy discount losartan on line, use a low dosage for the first 14 days of therapy diabetes mellitus oms buy 50 mg losartan overnight delivery, and then improve the dosage if rash has not occurred ketonuria diabetes mellitus type 2 buy losartan 50 mg mastercard. If extreme symptoms happen (eg diabetes medications for nurses losartan 25mg otc, delu- sufferers to contact their supplier instantly if they start feeling unhappy, hopeless, or suicidal. Inform ladies concerning the potential for fetal hurt, and instruct them to use a barrier method of birth control (eg, condom) in conjunction with a hormonal methodology (eg, oral contraceptive). Nevirapine induces cytochrome P450 and might thereby lower levels of different medicine. Effects on protease inhibitors, hormonal contraceptives, and methadone are of particular concern. To keep away from toxicity from extreme drug ranges, sufferers must not take cisapride, alprazolam, midazolam, triazolam, lovastatin, or simvastatin-or astemizole or terfenadine, that are now not available in the United States. In addition, the following drugs ought to be used with warning: indinavir, saquinavir, clarithromycin, dapsone, warfarin, quinidine, ergot alkaloids, phosphodiesterase type 5 inhibitors (eg, sildenafil [Viagra]), and the dihydropyridine-type calcium channel blockers. Antacids, histamine2-receptor blockers, proton pump inhibitors, and buffered formulations of didanosine can decrease absorption of delavirdine. Efavirenz competes with different drugs for metabolism by P450, and can thereby enhance their levels. To keep away from toxicity from excessive drug levels, the patient must not take astemizole, terfenadine, cisapride, midazolam, triazolam, dihydroergotamine, or ergotamine. Etravirine competes with other drugs for metabolism by P450 and can thereby enhance their ranges. All of the following drugs considerably scale back rilpivirine levels and hence are contraindicated: (1) antiseizure drugs (carbamazepine, oxcarbazepine, phenobarbital, phenytoin); (2) rifamycins (rifabutin, rifampin, rifapentine); (3) proton pump inhibitors (esomeprazole, lansoprazole, omeprazole, pantoprazole, rabeprazole); (4) glucocorticoids (when given in repeated doses); and (5) St. Antacids (eg, aluminum hydroxide, magnesium hydroxide, calcium carbonate) can scale back rilpivirine ranges. Advise sufferers to take antacids no less than 2 hours before rilpivirine or four hours after. Instruct sufferers of child-bearing potential to use a barrier contraceptive in addition to any hormonal contraceptive. Identifying High-Risk Patients Lopinavir/ritonavir oral answer is contraindicated for fullterm infants (until 14 days after birth) and preterm infants (until 14 days after their predicted due date). Instruct sufferers to take atazanavir with food, and to store it at room temperature. Instruct sufferers to take darunavir with meals, and to retailer it at room temperature. Instruct sufferers to take fosamprenavir suspension without food, and to take fosamprenavir tablets without meals or with food. Instruct sufferers to administer indinavir both (1) with water however on an empty stomach (ie, 1 hour before a meal or 2 hours after) or (2) with skim milk, juice, tea, or a low-fat meal (eg, corn flakes with skim milk and sugar), to take histamine2 blockers a minimal of 12 hours before rilpivirine or 4 hours after. Histamine2-receptor blockers (eg, cimetidine, famotidine, ranitidine) can reduce rilpivirine ranges. Advise patients Azole antifungal medication (eg, ketoconazole, itraconazole, fluconazole) and macrolide antibiotics (eg, erythromycin, clarithromycin, troleandomycin) can improve rilpivirine levels. Instruct sufferers to retailer indinavir at room temperature within the bundle provided by the producer. Advise patients utilizing lopinavir/ ritonavir tablets to take the drug with or with out meals, and to retailer it at room temperature. Instruct sufferers using lopinavir/ritonavir resolution to take the drug with food, and to retailer it at room temperature short term (up to 2 months) or under refrigeration long term. Instruct sufferers to take nelfinavir with food, and to retailer it at room temperature. Instruct patients to mix the powder formulation with a small amount of water, milk, formulation, soy formula, soy milk, or dietary complement, however not with acidic meals or juices (eg, applesauce, apple juice, orange juice). Instruct patients to take ritonavir tablets with food, and to store them at room temperature. Instruct sufferers to take ritonavir capsules with food (if possible) and to retailer unopened bottles underneath refrigeration. Instruct sufferers to take the oral resolution with food (if possible) and to retailer it at room temperature, by no means cold. Instruct patients to take saquinavir with a meal (or within 2 hours after a meal), and to store it at room temperature. Advise patients to take tipranavir with meals (when mixed with ritonavir tablets), and to take tipranavir with or without meals (when combined with ritonavir capsules or solution). Advise sufferers to store tipranavir solution at room temperature, by no means cold, and to retailer unopened bottles of tipranavir capsules underneath refrigeration (opened bottles could also be saved at room temperature for 60 days). If drugs are given to lower lipid levels, two agents-lovastatin and simvastatin-should be averted. Protease inhibitors may enhance the chance of bleeding in patients with hemophilia. Exercise warning in patients with chronic liver disease (eg, hepatitis B or C, cirrhosis). Instruct patients to report signs: pain in the stomach, groin, testicles, or facet of the again. To decrease the chance of nephrolithiasis, instruct sufferers to eat a minimal of forty eight ounces (1. To detect new-onset diabetes, measure blood glucose at baseline, every three to four months in the course of the first yr of therapy, and fewer regularly thereafter. Diabetes can be treated with insulin and oral antidiabetic brokers (eg, metformin). Diarrhea can usually be managed with loperamide or another over-the-counter antidiarrheal drug. Lopinavir/ritonavir oral solution may be deadly to newborns, owing to its propylene glycol content. Atazanavir and indinavir can raise plasma levels of unconjugated bilirubin (indirect bilirubin). Be alert for jaundice (yellowing of the skin) and icterus (yellowing of the eyes), which reverse upon drug withdrawal. To scale back risk, encourage patients to ensure sufficient intake of calcium and vitamin D. Accordingly, inform patients Preparation and Storage Teach patients to reconstitute powdered enfuvirtide with 1. To avoid severe toxicity from excessive drug levels, sufferers must not take cisapride, alprazolam, triazolam, midazolam, ergot alkaloids, lovastatin, or simvastatin-or astemizole or terfenadine, that are no longer obtainable within the United States. Buffered formulations of didanosine lower absorption of indinavir and ritonavir. Accordingly, buffered didanosine should be administered 1 or 2 hours other than these drugs. Fosamprenavir, lopinavir/ritonavir, nelfinavir, ritonavir, and tipranavir/ritonavir can scale back ranges of ethinyl estradiol, a part of many oral contraceptives. Inform patients about signs of pneumonia- cough, fever, and respiration difficulties-and instruct them to report these instantly. Enfuvirtide might trigger hypersensitivity reactions, manifesting as rash, fever, nausea, vomiting, chills, rigors, hypotension, or elevated serum transaminases, or presumably as respiratory misery, glomerulonephritis, Guillain-Barr� syndrome, or main immune complex reaction. Inform sufferers about indicators of hypersensitivity, and advise them to report them instantly. If a systemic hypersensitivity reaction happens, enfuvirtide must be discontinued and by no means used once more. Identifying High-Risk Patients Patients with elevated liver function and heart problems have to be monitored rigorously. Advise patients that, if they overlook to take a dose, to take the missed dose as quickly as potential, and take the following scheduled dose at its regular time. If the time to the next dose is less than 6 hours, the affected person ought to skip the missed dose and take the subsequent dose as scheduled. Raltegravir could cause doubtlessly fatal hypersensitivity reactions, together with Stevens-Johnson syndrome and toxic epidermal necrolysis. Inform sufferers about signs of a hypersensitivity reaction (eg, extreme rash, or rash associated with blisters, fever, malaise, fatigue, oral lesions, facial edema, hepatitis, angioedema, or muscle or joint aches), and instruct them to discontinue raltegravir immediately. Liver harm has been seen in some patients, and could additionally be preceded by evidence of an allergic reaction.
Order generic losartan on-line
Two measures-avoiding local consuming water and thoroughly washing foods-are highly efficient definition diabetes mellitus zuckerkrankheit buy discount losartan 50mg. Clostridium difficile is a gram-positive blood sugar vs a1c discount losartan online american express, anaerobic bacillus that infects the bowel diabetes type 1 etiology generic 50mg losartan amex. Symptoms range from relatively delicate (abdominal discomfort diabetic diet 1500 calories discount 25 mg losartan free shipping, nausea, fever, diarrhea) to very extreme (toxic megacolon, pseudomembranous colitis, colon perforation, sepsis, and death). The direct medical prices are estimated at $8 billion a yr; the indirect costs are much higher-about $25 billion a year. Infectious diarrhea could also be produced by enteric an infection with a variety of micro organism and protozoa. Indiscriminate use of antibiotics is undesirable in that it (1) can promote emergence of antibiotic resistance and (2) can produce an asymptomatic carrier state by killing most, but not all, of the infectious brokers. Despite extensive research, no underlying pathophysiologic mechanism has been identified. In addition, we all know that symptoms could be triggered by stress, depression, and dietary components, including caffeine, alcohol, fried meals, high-fat meals, gas-generating greens (beans, broccoli, cabbage), and too much sorbitol, a sweetener present in chewing gum and some food regimen merchandise. Overproduction of gastric acid and excessive bacterial colonization of the small intestine have additionally been implicated. Because giant meals stretch and stimulate the bowel, switching to smaller, more frequent meals could help. Another examine evaluated the impression of medicine that suppress manufacturing of stomach acid in sufferers who routinely experienced exacerbation of symptoms after eating. Two sorts of acid suppressants were used: proton pump inhibitors (lansoprazole or omeprazole) and histamine2 receptor blockers (famotidine or ranitidine). In all instances, sufferers experienced a big discount of postprandial urgency and other signs. Benefits developed rapidly (within days) and reversed when the drugs have been stopped. Owing to a threat of serious cardiovascular events, certainly one of these drugs- tegaserod-is used hardly ever, and then solely in emergency conditions. Regarding antispasmodic agents, they concluded that the obtainable data are inadequate to make a suggestion for or in opposition to use. Studies suggest that, for some patients, signs may be relieved with antibiotics or an acid suppressant. To scale back risk, prescribers, patients, and pharmacists must adhere to a strict threat management program (see below). As a result, the drug can improve stool firmness and reduce both fecal urgency and frequency. Symptoms decline 1 to four weeks after starting the drug, and resume 1 week after stopping the drug. Alosetron undergoes extensive metabolism by hepatic cytochrome P450 enzymes, adopted by excretion primarily within the urine. Although alosetron is usually well tolerated, it might possibly trigger extreme opposed results. The most typical downside is constipation (29%), which may be difficult by impaction, bowel obstruction, and perforation. In addition, alosetron can cause ischemic colitis (intestinal damage secondary to reduced blood flow). Ischemic colitis and issues of constipation have led to hospitalization, blood transfusion, surgical procedure, and death. If, after four weeks, the dosage is nicely tolerated however insufficient, it can be elevated to 1 mg twice a day. Patients who develop constipation or indicators of ischemic colitis (rectal bleeding, bloody diarrhea, new or worsening belly pain) ought to immediately inform the prescriber and discontinue the drug. Those with constipation may resume treatment, but solely after constipation has resolved, and solely on the recommendation of the prescriber. Unfortunately, benefits are modest: the drug can scale back stomach ache and discomfort, but solely in a small share of patients. As discussed in Chapter seventy nine, lubiprostone causes selective activation of chloride channels in epithelial cells of the gut, and thereby (1) promotes secretion of chloride-rich fluid into the intestinal lumen and (2) enhances motility of the small intestine and colon. Although tegaserod is approved for these sufferers, availability has been restricted by the manufacturer to emergency conditions. However, on April 2, 2008, the manufacturer-Novartis-decided to close the restricted access program. Tegaserod is rapidly absorbed, but bioavailability is low (about 10% in the absence of food and only 5% within the presence of food). Tegaserod undergoes metabolism to inactive products adopted by excretion in the bile. The most common opposed impact is diarrhea, which has been severe in some patients, resulting in dehydration, hypovolemia, and hypotension. Most cases happen in the course of the first week of treatment and resolve despite continued drug use. Because of the potential for cardiovascular harm, entry to tegaserod is restricted. Patients who develop indicators of ischemic colitis (eg, rectal bleeding, bloody diarrhea, new or worsening abdominal pain) should discontinue tegaserod and endure quick diagnostic testing. Tegaserod is contraindicated for women with known heart problems, severe renal impairment, reasonable or severe hepatic impairment, a history of bowel obstruction, symptomatic gallbladder illness, abdominal adhesions, or sphincter of Oddi dysfunction. Whereas tegaserod will increase intestinal motility and secretions, alosetron decreases motility and secretions. The beneficial initial dosage is 6 mg twice daily (taken at least 30 minutes earlier than meals) for 4 to 6 weeks. Ulcerative colitis is characterized by inflammation of the mucosa and submucosa of the colon and rectum. Five types of medication are employed: 5-aminosalicylates (eg, sulfasalazine), glucocorticoids (eg, hydrocortisone), immunosuppressants (eg, azathioprine), immunomodulators (eg, infliximab), and antibiotics (eg, metronidazole). Four aminosalicylates can be found: sulfasalazine, mesalamine, olsalazine, and balsalazide. Sulfasalazine [Azulfidine] belongs to the identical chemical household because the sulfonamide antibiotics. Sulfasalazine is handiest towards acute episodes of gentle to moderate ulcerative colitis. Hematologic disorders (eg, agranulocytosis, hemolytic anemia, macrocytic anemia) may happen. Sulfasalazine [Azulfidine] is available in 500-mg immediate- and delayed-release oral tablets. Mesalamine may be administered by retention enema, by rectal suppository, or by mouth (in tablets and capsules that dissolve after they reach the terminal ileum). The most common adverse impact is watery diarrhea, which occurs in 17% of sufferers. Balsalazide [Colazal] is an aminosalicylate indicated for mildly to moderately active ulcerative colitis. The commonest opposed effects are headache, belly pain, diarrhea, and nausea. Glucocorticoids are indicated primarily for induction of remission-not for long-term maintenance. Major opposed results are pancreatitis and neutropenia (secondary to bone marrow suppression). The fundamental pharmacology of azathioprine and mercaptopurine is mentioned in Chapters sixty nine and 102, respectively. Cyclosporine [Sandimmune, Neoral, Gengraf] is a stronger immunosuppressant than azathioprine or mercaptopurine, and acts sooner too. Cyclosporine is a probably poisonous compound that can cause renal impairment, neurotoxicity, and generalized suppression of the immune system. Because the doses employed are low (25 mg once a week), the toxicity associated with highdose therapy in cancer sufferers is averted. Systemic results are lower than with different glucocorticoids as a end result of absorbed budesonide undergoes in depth first-pass metabolism.
Order losartan 25 mg free shipping
Therapeutic and Diagnostic Applications the mydriatic functions of phenylephrine are very like these of the anticholinergic medication metabolic disease caused by impaired oxidation of fats order losartan american express. Phenylephrine-induced mydriasis is used as an help to intraocular surgery diabetic ketoacidosis symptoms purchase losartan pills in toronto, measurement of refraction diabetic diet 30 day menu order losartan with paypal, and ophthalmoscopic examination diabetic diet sugar intake buy discount losartan 50mg on-line. In patients with anterior uveitis, phenylephrine is given to dilate the pupil as part of an overall program of treatment. Like the anticholinergic drugs, phenylephrine can precipitate angle-closure glaucoma secondary to induction of mydriasis. Contraction of the dilator muscle could dislodge pigment granules from degenerating cells of the iris. These granules, which seem as "floaters" in the anterior chamber, are normally cleared from the eye inside a day. Rarely, topical phenylephrine is absorbed in quantities adequate to produce systemic toxicity. Cardiovascular responses (eg, hypertension, ventricular dysrhythmias, cardiac arrest) are of best concern. Other systemic reactions embody sweating, blanching, tremor, agitation, and confusion. Mast-cell stabilizers (eg, cromolyn, lodoxamide) stop release of inflammatory mediators. Patients ought to be informed that benefits take a quantity of days to develop, and several other weeks to turn out to be maximal. In distinction to mast-cell stabilizers, histamine1 (H1)-receptor antagonists (antihistamines) can provide quick symptomatic relief. Some medication (eg, azelastine, olopatadine) have two actions: They prevent mediator launch from mast cells and they block H1 receptors. The ocular decongestants (eg, naphazoline, phenylephrine) lower redness and edema by activating alpha1-adrenergic receptors on blood vessels, thereby inflicting vasoconstriction. Symptoms end result from harm to the macula, the central part of the retina that accommodates the best density of photoreceptors, and hence supplies the highresolution central imaginative and prescient used for reading, driving, stitching, recognizing faces, and so forth. The disease is characterised by the looks of drusen (yellow deposits under the retina). Initially, signs are attributable to launch of inflammatory mediators-histamine, prostaglandins, leukotrienes, and kinins-from mast cells. These mediators stimulate mucus manufacturing (and thereby trigger discharge), activate nerve endings (and thereby cause itching and burning sensations), and promote vasodilation and increase capillary permeability (and thereby cause redness and congestion). These symptoms peak about 20 minutes after allergen exposure and abate 20 minutes later. The late section is due to recruitment of immune cells-eosinophils, neutrophils, and macrophages-that amplify the inflammatory response. Fluid leakage lifts the macula from its regular place, which quickly causes everlasting harm. In addition, individuals took 2 mg of copper day by day to prevent copper deficiency anemia, which may develop after we devour lots of zinc. At this time, therapy with an angiogenesis inhibitor is preferred to the other two options. Administration is by direct injection into the vitreous humor of the affected eye. The largest concern is endophthalmitis, an irritation inside the attention brought on by bacterial, viral, or fungal an infection. Patients who experience symptoms (eg, redness, gentle sensitivity, pain) ought to search immediate medical consideration. All 4 drugs significantly cut back the chance of further visual impairment and development to blindness. In addition, research have proven that three agents-ranibizumab, bevacizumab, and aflibercept-can improve visible acuity that has been impaired. Laser Therapy In laser remedy, high-energy laser gentle is used to seal leaky blood vessels. First, laser mild can injury close by retinal tissue, and hence treatment is limited to regions away from the middle of the macula. Fourth, even when the process is done with due care, some loss of vision happens. This loss is justified by arguing that even greater loss would occur if therapy were withheld. As indicated, these agents differ with regard to structure, permitted utilization, cost, and efficacy. Two agents-ranibizumab and bevacizumab-are much like each other, and each differ from aflibercept and pegaptanib. For 5 days after the process, patients should shield their skin from daylight and shiny indoor light, because light-mediated activation of verteporfin in the skin might trigger a severe burn. Artificial tears are indicated for relieving dry-eye syndromes and discomfort and dryness attributable to irritants, wind, and solar. Artificial tears are devoid of antagonistic results, and therefore could also be administered as often and so lengthy as desired. Topical cyclosporine ophthalmic emulsion [Restasis] is prescribed for dry eyes due to inflammation. It suppresses the immune response, thereby selling resumption of tear manufacturing. Class and Generic Name Fluoroquinolones Trade Name Besivance Ciloxan Zymar Zymaxid Quixin Moxeza, Vigamox Ocuflox Azasite Ilotycin Gentak, Garamycin Tobrex Formulation 0. These preparations are used to reduce redness of the attention caused by minor irritation. The adrenergic brokers employed as decongestants are phenylephrine, naphazoline, oxymetazoline, and tetrahydrozoline. When applied to the eye in the low concentrations found in decongestant products, adrenergic agonists not often cause adverse results. Azithromycin Erythromycin Aminoglycosides Gentamicin Tobramycin Sulfonamides Glucocorticoids Glucocorticoids are used for inflammatory disorders of the eye (eg, uveitis, iritis, conjunctivitis). In distinction, extended remedy could trigger cataracts, lowered visible acuity, and glaucoma. This agent is utilized to the surface of the attention to detect lesions of the corneal epithelium; intact areas of the cornea remain uncolored whereas abrasions and other defects turn bright green. Fluorescein can be used topically and intravenously to assess move of aqueous humor. Adverse results from systemic administration embody nausea, vomiting, paresthesias, and pruritus. Rose bengal is utilized topically to visualize abrasions of the corneal and conjunctival epithelium. Lissamine green, another topical dye, turns shiny green in the presence of conjunctival defects and dryness. Polymyxin B/bacitracin Polymyxin B/bacitracin/ neomycin Polymyxin B/gramicidin/ neomycin Polymyxin B/ trimethoprim Ointment Ointment Solution Solution Topical Drugs for Ocular Infections Topical medicine are available for treating viral and bacterial infections of the attention. Four antiviral drugs-trifluridine, vidarabine, ganciclovir, and idoxuridine-are employed. These medication are used to treat critical ophthalmic infections and to forestall an infection following ocular surgical procedure. In the absence of remedy, irreversible damage to the optic nerve occurs in 1 or 2 days. Atropine and other anticholinergic drugs cause cycloplegia by blocking muscarinic receptors on the ciliary muscle, and cause mydriasis by blocking muscarinic receptors on the iris sphincter. By paralyzing the ciliary muscle, anticholinergic drugs stop the attention from focusing for near imaginative and prescient. By paralyzing the iris sphincter, anticholinergic drugs forestall the pupil from constricting in response to bright gentle; photophobia results. Phenylephrine, an adrenergic agonist, causes mydriasis by stimulating alpha-adrenergic receptors on the radial (dilator) muscle of the iris.
Buy losartan overnight delivery
In a trial reported in 2005 diabetes mellitus type 2 dyslipidemia purchase losartan with a mastercard, chemotherapy alone-doxorubicin plus cyclophosphamide diabetic neuropathy icd 9 discount losartan 50mg overnight delivery, followed by paclitaxel-was compared with chemotherapy plus trastuzumab 55 diabetes diet order 50 mg losartan with mastercard. Adding trastuzumab to the regimen produced a significant enhance in 3-year disease-free survival (87% vs diabetes diet app purchase losartan in united states online. The principal concern with trastuzumab is cardiotoxicity, manifesting as ventricular dysfunction and congestive heart failure. In scientific trials, the incidence of symptomatic coronary heart failure was 7% with trastuzumab alone, and 28% when trastuzumab was combined with doxorubicin, a drug with distinguished cardiotoxic actions. Because of cardiotoxicity, trastuzumab ought to be used with warning in women with preexisting coronary heart illness. Concurrent use with doxorubicin and different anthracyclines should usually be avoided. Many sufferers expertise a flu-like syndrome, which additionally happens with different monoclonal antibodies. The syndrome develops in 40% of sufferers receiving their first infusion, after which diminishes with subsequent infusions. Treatment consists of a loading dose (4 mg/kg infused over a minimum of ninety minutes) followed by weekly maintenance doses for 12 to 18 weeks (2 mg/kg infused over 30 minutes). An various regimen makes use of a larger loading dose (8 mg/kg), and bigger but less frequent maintenance doses (6 mg/kg each 3 weeks). Like trastuzumab, ado-trastuzumab emtansine is just effective against tumors that overexpress human epidermal progress factor receptor 2. In one trial involving ladies with metastatic disease, therapy with ado-trastuzumab emtansine elevated overall survival by 30. When in contrast with a remedy routine of iapatinib and capecitabine, there were fewer vital events and a higher survival fee. Ado-trastuzumab emtansine may cause hepatotoxicity, cardiotoxicity, and neurotoxicity. The commonest reactions embody nausea, fatigue, musculoskeletal ache, headache, and constipation. Other common, but extra serious, reactions include thrombocytopenia, increases in liver function test results, anemia, and hypokalemia. Like trastuzumab, ado-trastuzumab emtansine could cause probably fatal hypersensitivity reactions, infusion reactions, and pulmonary events. If a patient experienced trastuzumabrelated infusion reactions, ado-trastuzumab emtansine should be avoided. If indicators of toxicity are noticed, the dose could additionally be decreased or held until enchancment is seen. Symptoms include urticaria, bronchospasm, angioedema, hypotension, dyspnea, wheezing, pleural effusions, pulmonary edema, and hypoxia requiring oxygen. Most severe reactions developed in affiliation with the primary dose, either in the course of the infusion or by 12 hours after. Patients must be closely monitored for 60 minutes after the primary infusion, and for half-hour after subsequent infusions. Other opposed results embody cardiotoxicity, diarrhea, leukopenia, and neuropathy. Oligohydramnios has been reported in pregnancy, thus pregnant ladies should avoid use of pertuzumab. This is followed each 3 weeks by further infusions of 420 mg given over 30 to 60 minutes. The commonest opposed results of lapatinib plus letrozole are diarrhea, rash, nausea, and fatigue. Diarrhea happens in 65% of sufferers, and is the most typical purpose for stopping treatment. Accordingly, the drug ought to be used with warning in sufferers with present cardiac impairment. Liver function tests ought to be carried out at baseline and periodically all through treatment. When used alone and along with other drugs, letrozole has been associated with interstitial lung disease and pneumonitis. In laboratory animals, giving letrozole during pregnancy resulted in demise of the pups a couple of days after start. Lapatinib [Tykerb] is equipped in 250-mg tablets for oral dosing with out food (either 1 hour earlier than a meal or 1 hour after). Two dosing regimens are used: � � Lapatinib with capecitabine-The really helpful dosage is 1250 mg (5 tablets) taken as soon as every day, together with capecitabine Lapatinib with letrozole-The really helpful dosage is 1500 mg (6 tablets) taken once daily, together with letrozole (2. These metastases promote hypercalcemia by rising the activity of osteoclasts, the cells that promote bone resorption. Not only does resorption promote hypercalcemia, it weakens bone, and thereby will increase the chance of fractures. Fracture risk is further increased by use of antiestrogens and aromatase inhibitors. As we discussed in Chapter 61, estrogens promote bone health by inhibiting bone resorption and promoting bone deposition. Hence, by eradicating the influence of estrogen, the antiestrogens and aromatase inhibitors accelerate bone resorption and cut back bone deposition. Cytotoxic Drugs (Chemotherapy) Cytotoxic medicine could also be used earlier than breast surgical procedure or after. When used before surgery, chemotherapy can shrink large tumors, thereby allowing lumpectomy in ladies who would in any other case require a mastectomy. When used after surgery, chemotherapy can kill cancer cells that stay in the breast, in addition to cells which will have metastasized to distant websites. A common routine for breast cancer consists of doxorubicin (an anthracycline-type anticancer antibiotic) plus cyclophosphamide (an alkylating agent) adopted by paclitaxel (a mitotic inhibitor). Zoledronate and Other Bisphosphonates In girls with breast cancer, bisphosphonates may help protect bone integrity, and may thereby decrease the chance of hypercalcemia and fractures. At this time, two bisphosphonates-zoledronate [Zometa] and pamidronate [Aredia]-are approved for hypercalcemia of malignancy, and one of them-pamidronate-is also permitted for managing osteolytic bone metastases. Furthermore, compared with pamidronate, zoledronate has three benefits: onset is faster, length is longer, and infusion time is shorter (15 minutes vs. Principal adverse effects of the bisphosphonates are kidney injury and osteonecrosis of the jaw. In addition to lowering fractures and hypercalcemia, bisphosphonates may very well forestall metastases and prolong life. In girls with breast most cancers, bisphosphonates were originally employed to suppress bone resorption caused by metastases. While utilizing bisphosphonates for this objective, researchers famous something shocking: Bisphosphonates appeared to scale back the incidence of new bony metastases. Results of a follow-up examine confirmed the original remark: In girls with breast most cancers, remedy with a bisphosphonate lowered metastases to bone and prolonged survival. These outcomes have been obtained using clodronate, an oral bisphosphonate out there in Europe and Canada. When most cancers cells unfold to bone, they stimulate the exercise of osteoclasts, the cells answerable for bone resorption. In turn, osteoclasts release growth components that stimulate the most cancers cells, thereby setting up a self-reinforcing cycle. Bisphosphonates interrupt the cycle by inhibiting osteoclast operate and blocking tumor adhesion to bone. Efficacy was demonstrated in three double-blind trials that in contrast denosumab with zoledronate. One trial enrolled patients with breast most cancers, one enrolled sufferers with prostate most cancers, and one enrolled sufferers with other cancers, including a quantity of myeloma, kidney cancer, small cell lung most cancers, and non� small cell lung cancer. Principal opposed effects of denosumab are hypocalcemia, critical infections, pores and skin reactions, and osteonecrosis of the jaw. For males with localized prostate cancer, the popular remedies are surgical procedure and radiation, with or without adjunctive use of drugs. For men with metastatic prostate most cancers, drug therapy and castration are the one options.