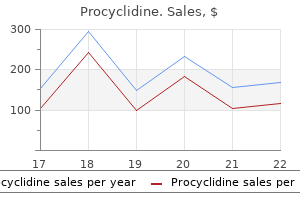
Procyclidine dosages: 5 mg
Procyclidine packs: 20 pills, 30 pills, 60 pills, 90 pills, 180 pills, 270 pills, 360 pills

Buy procyclidine 5mg cheap
The larger petrosal nerve passes anteriorly 897 treatment plant rd order discount procyclidine on line, receives a branch from the tympanic plexus and traverses a hiatus on the anterior floor of the petrous a part of the temporal bone medications parkinsons disease order procyclidine without a prescription. It enters the center cranial fossa symptoms 5 weeks into pregnancy order procyclidine 5mg on line, runs forwards in a groove on the bone above the lesser petrosal nerve treatment qt prolongation order procyclidine with a visa, after which passes beneath the trigeminal ganglion to attain the foramen lacerum. The higher petrosal nerve contains parasympathetic fibres destined for the pterygopalatine ganglion, and style fibres from the palate. The nerve to stapedius arises from the facial nerve within the facial nerve canal behind the pyramidal eminence of the posterior wall of the tympanic cavity and passes forwards through a small canal to reach the muscle. Branches from the plexus and the facial nerve supply buildings inside the tympanic cavity but in addition leave the cavity to provide constructions on the face. Tympanic plexus the nerves that represent the tympanic plexus ramify on the surface of the promontory on the medial wall of the tympanic cavity. The course of the style fibres from the mucous membrane of the palate and from the anterior presulcal part of the tongue is represented by the blue strains. Perigeniculate region: nerve compression and ischaemia are most likely to happen within the narrow meatal and labyrinthine segments, that are the vascular watershed areas of branches of the external carotid artery and the posterior circulation; the first genu is tethered by the larger petrosal nerve, rising susceptibility to shearing injuries; and the geniculate ganglion is susceptible to injury throughout surgical dissection in the supratubal recess of the anterior epitympanum. Tympanic section: the nerve is most incessantly dehiscent above the oval window; the distal tympanic phase and the second genu are both vulnerable to harm in cholesteatoma surgical procedure on account of pathological dehiscence or distorted anatomy and failure to determine essential surgical landmarks. Mastoid segment: the facial nerve is positioned lateral to the tympanic anulus and just distal to the stylomastoid foramen within the decrease portion of its vertical course and is subsequently prone to injury throughout surgical procedure involving the exterior acoustic meatus. It exits the skull on the petrotympanic fissure, and its additional course is described on page 552. The chorda tympani contains parasympathetic fibres that offer the submandibular and sublingual salivary glands by way of the submandibular ganglion and taste fibres from the anterior two-thirds of the tongue. Dehiscences of the facial nerve canal flaccid paralysis of the ipsilateral muscular tissues of facial expression; decreased lacrimation within the ipsilateral eye (which is controlled by neurones in the larger petrosal nerve); and hyperacusis or decreased tolerance of loud noises within the ipsilateral ear as a end result of paralysis of stapedius. Magnetic resonance imaging studies recommend that there are inflammatory changes in labyrinthine and perigeniculate segments of the facial nerve. In the vast majority of cases, spontaneous full recovery takes place after a few weeks. The facial nerve may be somewhat variable in its anatomical course through the temporal bone (Proctor and Nager 1982). The extra proximal the division into strands, the more bizarre is the subsequent course. It may be dehiscent, particularly in its second half, when it sometimes overhangs the stapes, or run inferior to the stapedial superstructure, a position that renders it susceptible throughout surgery to the stapes (Barnes et al 2001). The motor fibres to the face could also be carried via the chorda tympani, which is then enlarged. When that is the case, the distal facial nerve dwindles to a fibrous strand in a narrowed stylomastoid foramen. In persistent bone disease within the tympanic cavity, the facial nerve may be exposed in its canal. Inflammation may lead to facial paralysis of the infranuclear or decrease motor neurone kind. It is continuous with that of the pharynx, through the pharyngotympanic tube, and covers the ossicles, muscle tissue and nerves in the cavity to type the inside layer of the tympanic membrane and the outer layer of the secondary tympanic membrane. The middle ear mucosa is a mucus-secreting respiratory mucosa bearing cilia on its surface. The precise distribution of the mucociliary epithelium varies in regular middle ears, being more widespread in the younger. Three distinct mucociliary pathways have been recognized � epitympanic, promontorial and hypotympanic � the latter being the biggest. Each of these pathways coalesces on the tympanic orifice of the pharyngotympanic tube (Gleeson et al 1991). The mucosa types several vascular folds that extend from the tympanic walls to the ossicles: one descends from the roof of the cavity to the pinnacle of the malleus and the upper margin of the physique of the incus, and a second surrounds the stapedius. The folds separate off saccular recesses that give the inside of the tympanic cavity a somewhat honeycombed appearance; these mucosal folds have been described in greater detail by Proctor (1964). A, An indirect vertical section by way of the left temporal bone, to show the roof and lateral wall of the middle ear, the chorda tympani and the mastoid antrum. This area can play an important role within the retention of keratin and subsequent development of cholesteatoma. Cholesteatoma Cholesteatoma is the name given to keratinizing squamous epithelium within the middle ear. Theories embody development from embryological cell rests, metaplasia from inflamed mucoperiosteum, and aberrant migration of squamous epithelium either by way of a perforation in the tympanic membrane (usually in the pars flaccida or posterosuperior pars tensa) or within an space of tympanic membrane atelectasis the place the tympanic membrane turns into adherent to the medial wall of the tympanic cavity. A characteristic of cholesteatoma that continues to be poorly understood is its ability to erode bone, by activating osteoclasts, thus permitting the epithelium to proliferate and invade, destroying the temporal bone and carrying infection to the delicate tissues. Cholesteatoma can subsequently cause deafness through harm to the ossicles and internal ear; issues with balance through injury to the vestibule and semicircular canals; facial palsy by way of ischaemia and necrosis of the facial nerve; and intracranial sepsis. Treatment entails microsurgical dissection of the invading sac of epithelium with, wherever possible, preservation of the fragile structures just listed. A detailed anatomical description, emphasising the relations of the facial canal to adjacent buildings and variations in the middle of the canal. Barnes G, Liang J, Hall S et al 2001 Development of the Fallopian canal in people � a morphologic and radiologic examine. Bluestone C, Klein J 2002 Otitis media, atelectasis and Eustachian tube dysfunction. Campos A, Betancor L, Arias A et al 2000 Influence of human moist cerumen on the expansion of frequent and pathogenic bacteria of the ear. Gleeson M, Felix H, Neivergelt J 1991 Quantitative and qualitative analysis of the human center ear mucosa. Kawase T, Shibata S, Katori Y et al 2012 Elastic fiber-mediated enthesis within the human middle ear. Moschella F, Cordova A, Pirrello R et al 2003 the supra-auricular arterial community: anatomical bases for using superior pedicle retro-auricular pores and skin flaps. Proctor B 1964 the event of the center ear areas and their surgical significance. Purkait R 2013 Progression of growth within the exterior ear from delivery to maturity: a 2-year follow-up examine in India. All are positioned inside the labyrinth, a series of interlinked cavities within the petrous temporal bone containing interconnected membranous sacs and ducts. The different sacs include sensory epithelia consisting of supporting cells and mechanosensory cells, the hair cells that underlie acoustico-lateralis sensory techniques in all vertebrates. In humans, there are six such mechanosensory epithelia: the organ of Corti inside the cochlea (the hearing organ); the utricle and saccule (static stability organs); and the cristae of the semicircular canals (dynamic stability organs). Whilst sharing the identical basic structure, hair cells and the accent methods that encompass them show particular variations to each of the completely different sensory modalities. The inside acoustic meatus (internal auditory canal) and bony and membranous labyrinths are described here. The hole between the inner wall of the osseous labyrinth and the exterior surface of the membranous labyrinth is crammed with perilymph, a transparent fluid with an ionic composition much like that of different extracellular fluids, i. The membranous labyrinth incorporates endolymph, a fluid with an ionic composition extra like that of cytosol, i. These differences in ionic composition and potential, maintained by homeostatic tissues in the partitions of the labyrinth, are important to maximize the sensitivity of the mechanosensory hair cells that convert the vibrations set up in the internal ear fluids by head or sound movements into electrical indicators which might be transmitted through the vestibulocochlear nerve to the vestibular and cochlear nuclei, respectively, within the brainstem. It is considerably ovoid in shape but flattened transversely, and (on average) measures 5 mm from entrance to back and vertically, and three mm throughout. In its lateral wall is the opening of the oval window (fenestra vestibuli), into which the bottom of the stapes inserts, and to which the bottom of the stapes is hooked up by an anular ligament. Behind the recess is an indirect vestibular crest, the anterior finish of which varieties the vestibular pyramid. This crest divides beneath to enclose a small depression, the cochlear recess, which is perforated by vestibulocochlear fascicles as they move to the vestibular end of the cochlear duct. The planes of similarly orientated canals of the 2 sides also confirmed some departure from being parallel: left anterior/right posterior 24. The similar observers (Curthoys et al 1977) also measured the scale of the canals.
Buy procyclidine 5mg lowest price
A tumour of the inferior parathyroid located throughout the fascial thyroid sheath may descend along the inferior thyroid veins anterior to the trachea into the superior mediastinum treatment urinary retention purchase procyclidine on line, whereas whether it is outdoors the sheath medicine x ed cost of procyclidine, it could lengthen posteroinferiorly behind the oesopha gus into the posterior mediastinum medications like zoloft discount procyclidine online. The superior parathyroids are normally dorsal medications prescribed for adhd order procyclidine mastercard, and the inferior parathyroids ventral, to the recurrent laryngeal nerves. Microstructure Each parathyroid gland has a thin connective tissue capsule with intra glandular septa however lacks distinct lobules. In childhood, the gland consists of wide, irregular, interconnecting columns of chief or principal cells separated by a dense plexus of fenestrated sinusoidal capillaries. After puberty, adipose tissue accumulates in the stroma and sometimes accounts for about onethird of the adult tissue mass, increas ing further with age. Chief cells differ ultrastructurally based on their degree of activity; lively chief cells have massive Golgi complexes with quite a few vesicles and small membranebound granules. In contrast to the thyroid, where the actions of adjoining follicular cells are coordinated, indi vidual chief cells of the parathyroid glands go through cycles of secre tory activity and rest independently, in accordance with serum calcium levels. A second cell sort, the oxyphil (eosinophil) cell, seems simply earlier than puberty and will increase in number with age. Oxyphil cells are larger than chief cells and contain extra cytoplasm, which stains deeply with eosin. Their nuclei are smaller and extra darkly staining than those of chief cells, and their cytoplasm is unusually rich in mitochondria. The func tional significance of oxyphil cells and their relationship to chief cells are unsure. Lymph vessels are numerous and associated with those of the thyroid and thymus glands. Root of the neck Cervical rib A small further rib (cervical rib) may develop in the root of the neck in affiliation with the seventh cervical vertebra. It is usually fibrous in nature, though in some cases it might have undergone ossification. A cervical rib could trigger compression of the subclavian artery and the lower roots of the brachial plexus, by which case affected people will complain of pain, paraesthesia and even pallor of the affected higher limb, a condition known as thoracic outlet syndrome. The occasional cooccurrence of rudimentary or absent twelfth ribs with cervical ribs indicates that a homeotic shift had occurred over a larger a half of the vertebral column in affected fetuses (Bots et al 2011). For additional studying on homeotic transformations of vertebrae, see Ten Broek et al (2012). It begins in the neck, level with the decrease border of the cricoid cartilage and the sixth cervical vertebra. It descends, largely anterior to the vertebral column, into the superior mediastinum. Generally vertical and median, it inclines to the left as far as the root of the neck, and in addition bends in an anteroposterior airplane to comply with the cervical curvature of the vertebral column. The vertebral column, longus colli and pre vertebral layer of deep cervical fascia are posterior, and the widespread carotid artery and posterior part of the thyroid gland are lateral on all sides. The recurrent laryngeal nerves ascend on both sides in or near the groove between the trachea and the oesophagus. The brachiocephalic veins are shaped by the union of the inner jugular and subclavian veins on the junction of the neck and thorax, behind the head of the clavicle. The essential anatomical landmark in orientating and understanding the basis of the neck is scalenus anterior, lined by the prevertebral layer of deep cervical fascia. Anteriorly lie sternocleidomastoid and subclavius, the intermediate tendon of omohyoid, the subclavian vein, branches from the thyrocervical trunk of the first a half of the subclavian artery (transverse cervical, suprascapular and ascending cervical arter ies), and the phrenic nerve. The nerve lies on the floor of scalenus anterior within the root of the neck, earlier than passing between it and the subclavian vein to enter the superior mediastinum, and is the anatomi cal key to figuring out the muscle intraoperatively. Posteriorly, the roots of the brachial plexus and the second part of the subclavian artery sepa fee scalenus anterior from scalenus medius. Pathologies that cause impingement on either brachial plexus or subclavian artery might current clinically as an higher limb compression syndrome. The suprapleural membrane and pleura are intimate posterior relations of scalenus an terior. On each side, the apical (cervical) pleura and the apex of the lung bulge up into the root of the neck. The height to which the apical pleura rises � as regards to the first pair of ribs and costal cartilages � varies in different individuals based on the obliquity of the thor acic inlet. Scalenus anterior covers the anterolateral a part of the dome of the pleura and separates it from the subclavian vein. The subclavian artery crosses the dome below its summit, instantly above the vein. The costocervical trunk arches backwards from the subclavian artery and crosses the summit of the dome; its superior intercostal department descends behind the dome, between the primary intercostal nerve laterally and the first thor acic sympathetic ganglion medially. Medial relations of scalenus anterior are longus colli and the inferior thyroid artery. The two muscles are separated by an angular interval by way of which the vertebral artery and vein move to gain entry to the foramen transversarium of the sixth cervical vertebra, and extra anteri orly the inferior thyroid artery arches from lateral to medial on its method to the thyroid gland. The cervical sympathetic chain and the inferior cervical ganglion lie near the posteromedial side of the vertebral artery right here. The inner thoracic artery descends from the first a half of the subclavian artery; it passes behind the brachiocephalic vein and, on the right facet, is crossed by the phrenic nerve. The vagus descends anter ior to the primary part of the subclavian artery; on the proper facet only, its recurrent laryngeal branch normally turns across the decrease border of the artery. The terminal portions of the thoracic duct and the proper lym phatic duct, on the left and right sides, respectively, cross the triangular interval on the stage of the seventh cervical vertebra, coming into contact with the medial edge of scalenus anterior. The axillary sheath, an extension of the prevertebral fascia that accompanies the axillary artery and trunks of the brachial plexus, lies lateral to scalenus anterior. Vascular supply and lymphatic drainage the cervical a half of the oesophagus is principally equipped by branches from the inferior thyroid arteries. The oesophageal veins drain into the brachiocephalic veins, and lymphatic vessels pass to retropharyngeal, paratracheal or deep cervical lymph nodes. Innervation the cervical a part of the oesophagus is innervated by the recurrent laryngeal nerves and by the sympathetic plexus around the inferior thyroid artery. Anteriorly, the cervical a part of the trachea is crossed by skin and by the superficial and deep fasciae. It is also crossed by the jugular arch and overlapped by sternohyoid and sternothyroid. The second to fourth tracheal cartilages are crossed by the isthmus of the thyroid gland, above which an anastomotic artery connects the bilateral superior thyroid arteries. Below and in front are the pretracheal fascia, inferior thyroid veins, thymic remnants and the arteria thyroidea ima (when it exists). In kids, the brachiocephalic artery crosses obliquely in entrance of the trachea at or a little above the higher border of the manubrium. The oesophagus lies posterior to the trachea and sepa charges it from the vertebral column. The paired lobes of the thyroid gland, which descend to the fifth or sixth tracheal cartilage, and the common carotid and inferior thyroid arteries all lie lateral to the trachea. The recurrent laryngeal nerves ascend on each side, in or near the grooves between the sides of the trachea and oesophagus. The tracheal veins drain into the brachiocephalic veins through the inferior thyroid plexus, and lymphatic vessels drain into the pretracheal and paratracheal nodes. For detailed descriptions of the operative procedures, applicable surgical texts ought to be consulted. It is price emphasizing right here, nevertheless, the importance of understanding the relevant regional anatomy. In making a surgical airway, potential hazards can be averted by dissecting in the midline. In the midline, the isthmus of the thyroid gland, which normally overlies the second and third tracheal rings, must be divided. A high bifurcation of the brachio cephalic trunk, or aberrant anterior jugular veins (which usually lie between the midline and anterior border of sternocleidomastoid) are extra anatomical problems (Ger and Evans 1993, Jarvis 1966, Racic et al 2005). Cricothyroidotomy endangers the cricothyroid artery (a branch of the superior thyroid artery), which is often discovered close to the midline, and which reaches the median cricothyroid ligament close to the thyroid cartilage. Innervation the trachea is innervated by branches from the vagi, recurrent laryngeal nerves and sympathetic trunks.
Buy genuine procyclidine on line
The artery comes out of a fissure (erroneously termed a foramen) internal medicine purchase discount procyclidine online, and usually divides earlier than it enters the nasal cavity behind the crista ethmoidalis into posterior lateral nasal and posterior septal branches symptoms bladder cancer purchase 5mg procyclidine with mastercard. The number and distribution of its branches present great variation symptoms 8 dpo purchase 5 mg procyclidine free shipping, with a median of three or 4 branches (Babin et al 2003) treatment arthritis cheap procyclidine uk. The greater palatine department of the maxillary artery supplies the area of the inferior meatus. A department crosses the sphenoidal rostrum, beneath its natural ostium, to provide the nasal septum. This is utilized to provide pedicled, vascularized nasoseptal flaps in skull-base reconstruction. Its terminal half ascends by way of the incisive canal to anastomose on the septum with branches of the sphenopalatine and anterior ethmoidal arteries, and with the septal branch of the superior labial artery. The infraorbital artery and the superior, anterior and posterior alveolar branches of the maxillary artery provide the mucosa of the maxillary sinus. Turnover of olfactory receptor neurones Olfactory receptor neurones are lost and changed throughout life. Individual receptor cells have a variable lifespan, thought to common 1�3 months. Stem cells located near the bottom of the epithelium undergo periodic mitotic division throughout life, giving rise to new olfactory receptor neurones, which then develop a dendrite to the olfactory floor and an axon to the olfactory bulb. The cell our bodies of these new receptor neurones steadily move apically until they reach the area just under the supporting cell nuclei. When they degenerate, useless neurones either are shed from the epithelium or are phagocytosed by sustentacular cells. The fee of receptor cell loss and alternative will increase after exposure to damaging stimuli however declines slowly with age, a phenomenon that presumably contributes to diminishing olfactory sensory function in old age. Biopsy specimens from normosmic adults have revealed that patchy alternative of olfactory with respiratory epithelium happens even in younger healthy adults (Paik et al 1992, Holbrook et al 2005). In older patients, brisker bleeding might occur on account of the spontaneous rupture of arteries additional back within the nostril. These may be managed by making use of stress with a nasal pack, but the place this fails, knowledge of the pattern of arterial blood supply to the nasal cavity permits interruption of the appropriate blood supply by ligation or embolization of the feeding vessel. The sphenopalatine artery may be ligated under endoscopic visualization because it enters the nose by way of the sphenopalatine foramen. The ethmoidal arteries may be uncovered within the orbit and ligated to arrest bleeding excessive up within the nasal cavity. The maxillary artery may be exposed surgically behind the posterior wall of the maxillary sinus and ligated, or alternatively it might be recognized radiologically, utilizing a radiopaque dye, in order that it might be blocked by embolization (Simmen and Jones 2010). Numerous arteriovenous anastomoses are present in the deep layer of the mucosa and across the mucosal glands. The cavernous turbinate plexuses resemble these in erectile tissue; the nasal cavity is vulnerable to blockage, should they turn into engorged. Veins from the posterior part of the nostril usually cross to the sphenopalatine vein that runs back by way of the sphenopalatine foramen to drain into the pterygoid venous plexus. The anterior a half of the nose is drained primarily through veins accompanying the anterior ethmoidal arteries, and these veins subsequently cross into the ophthalmic or facial veins. Injection of vasoconstrictive brokers or corticosteroids throughout surgical procedure, notably to the inferior turbinates, could allow entry to the intracranial and ophthalmic circulations. A few veins move via the cribriform plate to connect with those on the orbital floor of the frontal lobes of the mind. When the foramen caecum is patent, it transmits a vein from the nasal cavity to the superior sagittal sinus. Lymphatic drainage Lymph vessels from the anterior area of the nasal cavity pass superficially to be a part of those draining the external nasal skin and finish within the submandibular nodes. The remainder of the nasal cavity, paranasal sinuses, nasopharynx and pharyngeal end of the pharyngotympanic tube all drain to the higher deep cervical nodes, both instantly or by way of the retropharyngeal nodes. Trigeminal fibres close to, and within, the epithelial layer are delicate to noxious chemicals. Autonomic fibres innervate mucous glands and control cyclical and reactive vasomotor activity. It provides off a lateral inner branch to supply the anterior part of the lateral wall, and a medial inside department to the anterior and upper components of the septum, earlier than emerging at the inferior margin of the nasal bone as the exterior nasal nerve to provide the pores and skin of the exterior nose to the nasal tip; damage following nasal trauma could lead to paraesthesia of the tip. The canal enters the pterygopalatine fossa, and the nerve joins the pterygopalatine ganglion, the place the parasympathetic fibres synapse, but the sympathetic fibres pass via without synapsing (Ch. The nerve of the pterygoid canal is a vital landmark to the petrous portion of the inner carotid artery, and may also hardly ever be transected to treat intractable rhinorrhoea. Sympathetic postganglionic vasomotor fibres are distributed to the nasal blood vessels. Postganglionic parasympathetic fibres derived from the pterygopalatine ganglion present the secretomotor supply to the nasal mucous glands, and are distributed by way of branches of the maxillary nerves. A 3 Olfactory nerves Olfactory nerves are bundles of very small axons derived from olfactory receptor neurones within the olfactory mucosa. The axons are unmyelinated, and in varying phases of maturity, reflecting the fixed turnover of olfactory neurones that takes place within the olfactory epithelium. Bundles of axons surrounded by olfactory ensheathing cells kind a plexiform community within the subepithelial lamina propria of the mucosa. The bundles unite into as many as 20 branches that cross the cribriform plate in lateral and medial groups, and enter the overlying olfactory bulb, the place they finish in glomeruli. The dura subsequently turns into continuous with the nasal periosteum, and the pia arachnoid merges with the connective tissue sheaths surrounding the nerve bundles, an association that may favour the unfold of an infection into the cranial cavity from the nasal cavity. In extreme accidents involving the anterior cranial fossa, the olfactory bulb could additionally be separated from the olfactory nerves or the nerves may be torn, producing anosmia, i. Fractures could involve the meninges, in order that cerebrospinal fluid might leak into the nostril, resulting in cerebrospinal rhinorrhoea. They all open into the lateral wall of the nasal cavity by small apertures that allow each the equilibration of air between the varied air spaces and the clearance of mucus from the sinuses into the nostril by way of a mucociliary escalator. The detailed place of these apertures, and the precise type and size of every of the sinuses, range enormously between individuals (Lang 1989, Beale et al 2009, Navarro 1997). Respiratory epithelium extends via the apertures of the paranasal sinuses to line their cavities, a feature that sadly favours the spread of infections. Sinus mucosa is thinner and less vascular, and has fewer goblet cells, than nasal mucosa. Cilia are at all times current in the mucosa close to the apertures however less evenly distributed elsewhere inside the sinuses. They clearly add some resonance to the voice, and in addition enable the enlargement of native areas of the skull while minimizing a corresponding enhance in bony mass. It is likely that such growth-related changes serve to strengthen particular regions. In many macrosomatic animals, the vomeronasal organ consists of a vomeronasal duct that accommodates chemosensory cells, and a vomeronasal nerve that terminates centrally within the accessory olfactory bulb. The vomeronasal organ exists in the developing human fetus but its existence in the adult has lengthy been controversial. The regular orifice of the maxillary sinus is proven on the proper facet and an accessory orifice on the left aspect. Foramen rotundum Anterior clinoid course of Understanding the development of the sinuses at every stage of childhood is crucial for interpreting pathology and planning surgery. Cadaveric and radiological research have offered normative information for sinus improvement. Each normally underlies a triangular area on the surface of the face, its angles formed by the nasion, a point 3 cm above the nasion and the junction of the medial third and lateral two-thirds of the supraorbital margin. The two sinuses are rarely symmetric, since the septum between them often deviates from the median aircraft. Each sinus may be additional divided into numerous speaking recesses by incomplete bony septa. Each often has a frontal portion that extends upwards above the medial a half of the eyebrow, and an orbital portion that extends again into the medial part of the roof of the orbit. One or both sinuses might not often be hypoplastic and even absent; racial differences have been reported. Most sinuses are rudimentary or absent at start, but enlarge appreciably during the eruption of the permanent tooth and after puberty, occasions that significantly alter the dimensions and form of the face. The uncinate, hiatus semilunaris and ethmoidal bulla are already well-defined, fastened landmarks, and each the anterior and posterior ethmoidal cells are already nearly utterly developed in terms of quantity but not dimension. The cells are separated by connective tissue, which turns into compressed with subsequent expansion of the cells.
Generic 5mg procyclidine fast delivery
The trabecular inside accommodates pink bone marrow and one or two giant ventrodorsal canals that include the basivertebral veins medicine dictionary pill identification best purchase for procyclidine. Pubertal adolescents have higher trabecular bone density than prepubertal youngsters medicine woman cast 5mg procyclidine overnight delivery. Sexual dimorphism in vertebrae has obtained little consideration treatment efficacy buy procyclidine master card, but Taylor and Twomey (1984) have described radiological variations in adolescent people and have reported that female vertebral bodies have a decrease ratio of width to depth medicine x boston buy 5 mg procyclidine visa. Vertebral body diameter has additionally been used as a foundation for intercourse prediction within the evaluation of skeletal materials (MacLaughlin and Oldale 1992). Key: 1, bone derived from anular epiphysis; 2, vertebral physique � bone derived from centrum; three, pedicle; 4, superior articular aspect; 5, transverse course of; 6, spinous process; 7, vertebral body � bone derived from neural arch; eight, vertebral foramen; 9, costal side; 10, lamina. These differences in texture reflect variations within the early construction of intervertebral discs. In the horizontal airplane, the profiles of most our bodies are convex anteriorly, but concave posteriorly the place they complete the vertebral foramen. There is some variation in measurement of the last two lumbar bodies, however thereafter width diminishes quickly to the coccygeal apex. On each side, the vertebral arch has a vertically narrower ventral part � the pedicle � and a broader lamina dorsally. Paired transverse, superior and inferior articular processes project from their junctions. These variations are matched by variations within the diameter of the spinal cord and its enlargements. In the lumbar area, the vertebral canal decreases steadily in dimension between L1 and L5, with a greater relative width in the female. These are a central zone, between the medial margins of the side joints, and two lateral zones, beneath the side joints and getting into the intervertebral foramina. Each lateral zone, which passes into and just past the intervertebral foramen, could be further subdivided into subarticular (lateral recess), foraminal and extraforaminal areas (MacNab and McCulloch 1990). The central zone of the canal is somewhat narrower than the radiological interpedicular distance if the lateral recess is taken into account to be part of the radicular canal quite than part of the central zone. The thoracic and lumbar intervertebral foramina face laterally and their transverse processes are posterior. In addition, the anteroinferior boundaries of the primary to tenth thoracic foramina are shaped by the articulations of the head of a rib and the capsules of double synovial joints (with the demifacets on adjacent vertebrae and the intra-articular ligament between the costocapitular ridge and the intervertebral symphysis). Lumbar foramina lie between the 2 principal lines of vertebral attachment of psoas major. The partitions of each foramen are coated throughout by fibrous tissue, which is in flip periosteal (though the presence of a true periosteum lining the vertebral canal is controversial: Newell (1999)), perichondrial, anular and capsular. The more lateral parts of the foramina could also be crossed at a variable degree by slender fibrous bands, the transforaminal ligaments (for element of these ligaments, see Bogduk (2005)). A foramen accommodates a segmental mixed spinal nerve and its sheaths, from two to 4 recurrent meningeal (sinuvertebral) nerves, variable numbers of spinal arteries, and plexiform venous connections between the inner and exterior vertebral venous plexuses. These structures, significantly the nerves, could also be affected by trauma or one of many many issues that will affect tissues bordering the foramen. This lower may result from facet joint osteoarthritis, osteophyte formation, disc degeneration and degenerative spondylolisthesis, all of which may lead to lateral or foraminal spinal stenosis. There is a developmental type of the condition that primarily impacts the central canal but extra commonly the stenosis is degenerative, and results from intervertebral disc narrowing and osteoarthritic changes in the facet joints. The lumbosacral intervertebral foramen, which is normally the smallest within the area, is especially liable to such stenosis. Severe spinal stenosis might compress the spinal wire and compromise its arterial provide. Ischaemia of the nerves and roots could provoke extra injury than the precise physical compression of the neural tissue. The first, second and seventh have particular options and will be considered individually. The third, fourth and fifth cervical are almost identical, and the sixth, whereas typical in its basic features, has minor distinguishing features. Because of their development, contents and susceptibilities to a number of issues, the intervertebral foramina are loci of nice biomechanical, useful and scientific significance. The specializations cranial to the axis and at sacral ranges are described with the individual bones and articulations. The pedicles connect halfway between the discal surfaces of the vertebral body, so the superior and inferior vertebral notches are of similar depth. The laminae are thin and slightly curved, with a skinny superior and slightly thicker inferior border. The transverse course of is morphologically composite around the foramen transversarium. The attachment of the dorsal bar to the pediculolaminar junction represents the morphological transverse course of, and the attachment of the ventral bar to the ventral physique represents the capitellar course of. In all however the seventh cervical vertebra, the foramen transversarium usually transmits the vertebral artery and vein and a branch from the cervicothoracic ganglion (vertebral nerve). The posterior floor is flat or minimally concave, and its discal margins give attachment to the posterior longitudinal ligament. The central space shows several vascular foramina, of which two are commonly comparatively bigger. These are the basivertebral foramina, which transmit basivertebral veins to the anterior inner vertebral plexus. The superior discal floor is saddle-shaped, formed by flange-like lips, uncinate processes, which arise from a lot of the lateral circumference of the upper margin of the vertebral body. Uncinate processes are rudimentary at delivery and are normally found on the third to seventh cervical vertebra in the adult. The uncinate processes on the vertebra under articulate with the corresponding bevelled surfaces on the inferior aspect of the vertebra above. The inferior discal surface can be concave; the concavity is produced primarily by a broad projection from the anterior margin, which partly overlaps the anterior surface of the intervertebral disc. The discal surfaces of cervical vertebrae are so shaped so as to prohibit each lateral and anteroposterior gliding actions throughout articulation. The paired ligamenta flava prolong from the superior border of every lamina below to the roughened inferior half of the anterior surfaces of the lamina above. The superior a half of the anterior floor of each lamina is clean, like the immediately adjacent surfaces of the pedicles, that are usually in direct contact with the dura mater and cervical root sheaths to which they may turn into loosely connected. The spinous process of the sixth cervical vertebra is bigger and is often not bifid. The superior articular aspects, flat and ovoid, are directed superoposteriorly, whereas the corresponding inferior sides are directed mainly anteriorly, and lie nearer the coronal plane than the superior facets. In youngsters, side joint angle decreases until 10 years of age and remains unchanged thereafter (Kasai et al 1996). The dorsal rami of the cervical spinal nerves curve posteriorly, close to the anterolateral aspects of the lateral plenty, and may very well lie in shallow grooves, especially on the third and fourth pairs. The dorsal root ganglion of every cervical spinal nerve lies between the superior and inferior vertebral notches of adjacent vertebrae. The large anterior ramus passes posterior to the vertebral artery, which lies on the concave higher floor of the costal lamella; the concavity of the lamellae will increase from the fourth to the sixth vertebra. The fourth to sixth anterior tubercles are elongated and rough for muscle attachment. The carotid artery could be forcibly compressed in the groove shaped by the vertebral bodies and the larger anterior tubercles, particularly the sixth. The posterior tubercles are rounded and more laterally placed than the anterior, and all but the sixth are additionally extra caudal; the sixth is at about the identical stage because the anterior. Key: 1, C1 posterior tubercle; 2, C2 spinous process; three, C3 inferior articular process; four, C4 lamina; 5, C6 superior articular aspect; 6, C6/7 aspect (zygapophyseal) joint. Key: 1, physique; 2, posterior tubercle of transverse course of; 3, pedicle; four, lamina; 5, bifid spinous course of; 6, anterior tubercle of transverse course of; 7, foramen transversarium; 8, superior articular aspect; 9, vertebral foramen. Key: 1, uncinate process; 2, body; three, anterior tubercle of transverse process; 4, posterior tubercle of transverse course of; 5, superior articular course of; 6, lateral mass; 7, lamina; 8, spinous course of; 9, inferior articular process. Tendinous slips of scalenus anterior, longus capitis and longus colli are hooked up to the fourth to sixth anterior tubercles.
Cheap 5 mg procyclidine otc
The presence of the oily symptoms 7 cheap procyclidine 5mg on-line, hydrophobic secretions of tarsal glands alongside the margins of the eyelids also inhibits the spillage of tears on to the face medicine 7253 purchase procyclidine 5mg amex. Obstruction of the tarsal gland ducts by lipid and cellular debris might end in lipogranulomatous irritation and the clinical manifestations of an inner hordeolum or chalazion symptoms xanax is prescribed for procyclidine 5 mg on line. Their branches course laterally along the tarsal edges to kind superior and inferior arcades (two within the higher eyelid and one in the lower) treatment jellyfish sting discount procyclidine 5mg online. The eyelids are also supplied by branches of the infraorbital, facial, transverse facial and superficial temporal arteries. The veins that drain the eyelids are bigger and more numerous than the arteries; they move either superficially to veins on the face and forehead, or deeply to the ophthalmic veins throughout the orbit. The lymph vessels that drain the eyelids and conjunctiva begin in a superficial plexus beneath the skin, and in a deep plexus in entrance of and behind the tarsi. These plexuses communicate with one another, and medial and lateral sets of vessels arise from them. The lateral lymph vessels drain the whole thickness of the lateral a half of the upper and lower lids, and cross laterally from the lateral canthus to finish in the superficial and deep parotid lymph nodes. The lymph vessels of the medial set drain the skin over the medial a part of the upper eyelid, the entire thickness of the medial half of the decrease lid, and the caruncle; they follow the course of the facial vein to end in the submandibular group of lymph nodes. The higher eyelid is supplied primarily by the supraorbital branch of the frontal nerve. Additional contributions come from the lacrimal nerve, the supratrochlear department of the frontal nerve, and the infratrochlear department of the nasociliary nerve. The nerve supply to the decrease eyelid is derived principally from the infraorbital department of the maxillary nerve, with small contributions from the lacrimal and infratrochlear nerves. Conjunctival goblet cells contribute the mucin component of the preocular tear film and play a central position within the defence of the ocular floor against microbial an infection. The marginal, tarsal and orbital areas are collectively referred to because the palpebral conjunctiva. The marginal zone extends from a line immediately posterior to the openings of the tarsal glands and passes across the eyelid margin to continue on the inside floor of the lid so far as the subtarsal groove (a shallow sulcus that marks the marginal border of the tarsus). The tarsal conjunctiva is highly vascular and is firmly attached to the underlying tarsal plate. The orbital zone extends so far as the fornices, which mark the road of reflection of the conjunctiva from the lids on to the eyeball. The conjunctiva is extra loosely connected to underlying tissues over the orbital zone and so folds readily. The bulbar conjunctiva is loosely connected to the eyeball over the exposed sclera, is skinny and transparent, and readily permits the visualization of conjunctival and episcleral blood vessels. At the free palpebral margins, the conjunctiva is continuous with the skin of the eyelids, the liner epithelium of the ducts of the tarsal glands, and with the lacrimal canaliculi and lacrimal sac (see below). The continuity between the conjunctiva and the nasolacrimal duct and nasal mucosa is essential in the spread of an infection. Fornix Orbital Bulbar the conjunctiva is composed of an epithelial layer and an underlying fibrous layer or substantia propria. The form of the epithelium and thickness of the substantia propria range with location. At the margin of the lids, the epithelium is non-keratinized stratified squamous and 10�12 cells thick. The epithelium of the tarsal conjunctiva thins to two or three layers and consists of columnar and flat surface cells. Near the fornices, the cells are taller, and a trilaminar conjunctival epithelium covers a lot of the bulbar conjunctiva. It thickens closer to the corneoscleral junction after which modifications to stratified squamous epithelium typical of the cornea. A proportion of limbal conjunctival epithelial cells function stem cells for the corneal epithelium; this region of the conjunctiva is therefore important for maintaining corneal integrity. They show a marked regional variation in density, being most frequent in conjunctival regions normally coated by the eyelids, and lowered in number inside uncovered interpalpebral locations (Doughty 2012). The substantia propria, or fibrous layer, is thickest at the fornix and thinnest over the tarsi where conjunctival attachment is firmest. With the exception of the tarsal conjunctiva, the substantia propria adjacent to the epithelium is principally loose. It merges with the fibrous fascia bulbi and episclera within the limbal and bulbar regions, and is loosely connected to the sheaths of the recti. Vascular provide and lymphatic drainage Limbal Tarsal Marginal the arteries of the palpebral conjunctiva are derived from the vascular arcades of the eyelids. Many of the small vessels of the eyelid drain to the conjunctival veins, which, in turn, pass again to the orbital and facial veins. A dense capillary community is arranged in a single subepithelial lamina, a distribution that meets the requirement of the cornea throughout sleep, when oxygen is on the market to the cornea only via this vascular system. The bulbar conjunctiva receives blood from the palpebral arcades and from the anterior ciliary arteries that reach the conjunctiva on the orbital surface of the recti. The conjunctiva is innervated by sensory nerves from the identical ophthalmic and maxillary branches of the trigeminal nerve that serve the eyelid. Autonomic nerve fibres are abundant within the conjunctiva, notably in bulbar and limbal regions, and are most likely vasomotor in function. It is distributed throughout the precorneal tear film (1�2 �l), and alongside the upper and decrease marginal tear strips (5�6 �l), which are wedge-shaped menisci that run along the posterior border of the lid margins and be part of collectively at the canthi. Lacrimal gland the lacrimal gland is the first producer of the aqueous element of the tear layer. Tears are produced by the lacrimal gland and move within the higher and decrease meniscus. Tears drain sequentially by way of the puncta, canaliculi, lacrimal sac and nasolacrimal duct. Acini encompass secretory cells that discharge their product right into a central lumen steady with an intercalated duct fashioned from a single layer of epithelial cells that lack secretory granules. Myoepithelial cells prolong processes across the perimeter of acini and ducts; their contraction imparts a mechanical drive on the acini and ducts, which promotes the expulsion of tears from the gland. The interstices of the gland are composed of free connective tissue that accommodates numerous immune cells, mainly B-lymphocytes and plasma cells (particularly IgA-secreting cells). The lacrimal gland consists of orbital and palpebral parts which might be continuous posterolaterally around the concave lateral edge of the aponeurosis of levator palpebrae superioris. The orbital part, about the measurement and form of an almond, lodges in a shallow fossa on the medial facet of the zygomatic strategy of the frontal bone, just within the orbital margin. Its decrease surface is linked to the sheath of levator palpebrae superioris and its upper surface is connected to the orbital periosteum. Its anterior border is in contact with the orbital septum and its posterior border attached to the orbital fat. The main ducts of the lacrimal gland, as a lot as 12 in number, discharge into the conjunctival sac on the superior lateral fornix. Those from the orbital half penetrate the aponeurosis of levator palpebrae superioris to be a part of those from the palpebral half. Excision of the palpebral half is therefore functionally equal to total elimination of the gland (Maitchouk et al 2000). Many small accent lacrimal glands (glands of Krause and Wolfring) occur in or near the fornix. Lacrimal gland Accessory lacrimal glands Innervation the lacrimal gland is innervated by secretomotor postganglionic parasympathetic fibres from the pterygopalatine ganglion (Ch. They attain the gland either through zygomatic and lacrimal branches of the maxillary nerve, or by passing directly from the ganglion (Ruskell 2004). Sympathetic fibres that issue from the superior cervical ganglion additionally supply the lacrimal gland. These fibres may be concerned in the regulation of blood move and the modulation of gland secretion (Dartt 2009). The afferent limb of the reflex includes branches of the ophthalmic nerve, with an additional contribution from the infraorbital nerve if the conjunctiva of the decrease eyelid is involved.
Buy procyclidine 5 mg overnight delivery
Traumatic scalp avulsion might occur if hair becomes trapped in shifting machinery or a shearing drive is utilized in the subgaleal aircraft throughout a street visitors accident or fall damage medications 122 discount 5 mg procyclidine visa. The arterial blood supply to the scalp is especially rich medications and mothers milk order 5 mg procyclidine otc, and there are free anastomoses between branches of the occipital and superficial temporal vessels medicine 81 procyclidine 5mg amex. Scalp lacerations continue to bleed profusely because the elastic fibres of the underlying galea aponeurotica stop preliminary vessel retraction symptoms brain tumor order procyclidine with amex. Their restore requires a twolayer closure method to approximate the galea aponeurotica and skin layers. Fibres of orbicularis oculi, corrugator and the frontal a part of occipitofrontalis are inserted into the dermis of the eyebrows. The exterior junction is indicated by the nasolabial groove (sulcus) and additional laterally by the nasolabial fold, which descends from the aspect of the nostril to the angle of the mouth. The cheek is roofed on the outer floor by pores and skin and on the inner surface by mucosa. Each cheek contains the buccinator muscle, and a variable, but usually appreciable, quantity of adipose tissue, which is usually encapsulated to type a biconcave mass, the buccal fat pad (of Bichat), significantly evident in infants. The corresponding reflexion within the decrease lip coincides roughly with the mentolabial sulcus, and right here the lip is steady with mental tissues. The higher and decrease lips differ in crosssectional profile in that neither is an easy fold of uniform thickness. The higher lip has a bulbous asymmetrical profile: the pores and skin and redlip have a slight exterior convexity, and the adjoining redlip and mucosa a pronounced inner convexity, making a mucosal ridge or shelf that can be wrapped across the incisal edges of the parted tooth. When lesions on the face, similar to scars, pigmented lesions and skin cancers, are excised, the scale of those lesions typically require exci sion as an ellipse, in order that the resulting defect could be closed as a straight line. If the ensuing scar is to be aesthetically acceptable, it could be very important make the lengthy axis of the ellipse parallel to the pure relaxed pores and skin pressure traces, in order that the scar will seem like a natural pores and skin crease. If the excision line runs contrary to the pores and skin tension strains, the scar may be more conspicuous and will are most likely to stretch transversely as a result of natural expressive facial movements. When bigger lesions are excised, it might be necessary to advance or rotate adjoining gentle tissue to fill the defect. The capability to raise these pores and skin flaps is entirely dependent on the regional blood provide, and each random pattern and axial sample skin flaps are used surgically. Because of the richness of the subdermal plexus within the face, random sample flaps can be raised with a larger size:breadth ratio than in some other area of the physique. The following are examples of axial sample flaps that can be used to reconstruct defects on the face and scalp. The frontal department of the superficial temporal artery anastomoses within the midline with its opposite quantity, and con sequently the whole brow pores and skin could be raised on a slim pedicle primarily based on just one of many superficial temporal arteries. The parietal department of the superficial temporal artery and the Fascial layers and tissue planes in the face On the premise of gross dissection and complementary histological studies, 4 distinct tissue planes are acknowledged on the face superficial to the airplane of the facial nerve and its branches. Subcutaneous fibroadipose tissue this homogeneous layer is current throughout the face, though the diploma of adiposity varies in several parts of the face and with age. Anteriorly, it crosses the nasolabial fold on to the lip; superiorly, it crosses the zygomatic arch. The fat content of the subcutaneous tissue in the cheek accounts for the cheek mass; a half of the subcutaneous adipose tissue is the malar fat pad, a more or less discrete aggregation of fatty tissue inferolateral to the orbital margin. When traced under the extent of the decrease border of the mandible, it becomes con tinuous with platysma within the neck. Microdissection has revealed that the superficial musculoaponeurotic system becomes indistinct on the lateral aspect of the face approximately 1 cm under the extent of the zygomatic arch. Anteromedially, the superficial musculoaponeurotic system layer turns into continuous with a variety of the mimetic muscular tissues, Bones of the facial skeleton and cranial vault including zygomaticus main, frontalis and the periorbital fibres of orbicularis oculi (Yousif and Mendelson 1995). In most areas of the face, a distinct subsuperficial musculo aponeurotic system aircraft could be outlined deep to the superficial musculoaponeurotic system. It is steady with the plane between platysma and the underlying investing layer of deep cervical fascia within the neck. However, where it overlies the parotid gland, the superficial musculoaponeurotic system is firmly blended with the superficial layer of the parotid fascia, which means that a clear subsuperficial musculo aponeurotic system plane is troublesome, if not unimaginable, to define in the area of the parotid. Below, at approximately the extent of the superior orbital rim, it splits into superficial and deep laminae that run downwards to attach to the lateral and medial margins of the higher floor of the zygomatic arch, respectively. These fascial connect ments have a clinical application within the reduction of fractures of the zygomatic complicated through a Gillies strategy: an instrument is inserted deep to the deep lamina of temporalis fascia via a scalp incision and used to elevate depressed zygomatic complicated fractures. The fat enclosed between these two layers is termed the superficial temporal fats pad; it incorporates the zygomaticoorbital branch of the superficial tem poral artery and a cutaneous nerve, the zygomaticotemporal department of the maxillary nerve. The temporal fascia is overlapped by auriculares anterior and superior, the epicranial aponeurosis and a half of orbicularis oculi, and the superficial temporal vessels and auriculotemporal nerve ascend over it. Parotid�masseteric fascia this is a skinny, translucent and hard fascial layer that covers the parotid duct and the buccal branch of the facial nerve and interconnecting branches from the mandibular nerve as these buildings all lie on the floor of masseter. Further anteriorly, the parotid�masseteric fascia overlies the buccal fats pad lying superficial to buccinator. Having crossed the floor of the buccal fats pad, the fascia blends with the epimysium on the floor of buccinator. It is steady with the investing layer of deep cervical fascia below the lower border of the mandible. Buccopharyngeal fascia the parotid gland is surrounded by a fibrous capsule called the parotid fascia or capsule. Traditionally, this has been described as an upward continuation of the investing layer of deep cervical fascia in the neck, which splits to enclose the gland within a superficial and a deep layer. The superficial layer is hooked up above to the zygomatic process of the temporal bone, the cartilaginous a part of the external acoustic meatus, and the mastoid process. The deep layer is attached to the mandible, and to the tympanic plate, styloid and mastoid processes of the tempo ral bone. The prevailing view is that the deep layer of the parotid capsule is derived from the deep cervical fascia. However, the superficial layer of the parotid capsule appears to be steady with the fascia associ ated with platysma, and is now thought to be a part of the super ficial musculoaponeurotic system (Mitz and Peyronie 1976, Wassef 1987, Gosain et al 1993). It varies in thickness from a thick fibrous layer anteriorly to a thin translucent membrane posteriorly. It could also be traced forwards as a separate layer which passes over the masseteric fascia (itself derived from the deep cervical fascia), separated from it by a cel lular layer that contains branches of the facial nerve and the parotid duct. Histologically, the parotid fascia is atypical in that it contains muscle fibres that parallel those of platysma, especially in the decrease part of the parotid capsule. The deep fascia covering the muscular tissues forming the parotid bed (digas tric and styloid group of muscles) contains the stylomandibular and mandibulostylohyoid ligaments. The stylomandibular ligament passes from the styloid process to the angle of the mandible. The more exten sive mandibulostylohyoid ligament (angular tract) passes between the angle of the mandible and the stylohyoid ligament for varying dis tances, usually reaching the hyoid bone. It is thick posteriorly but thins anteriorly within the region of the angle of the mandible. There is a few dispute as to whether the mandibulostylohyoid ligament is a part of the deep cervical fascia (Ziarah and Atkinson 1981) or lies deep to it (Shimada and Gasser 1988). The stylomandibular and mandibulo stylohyoid ligaments separate the parotid gland area from the super ficial part of the submandibular gland, and so are landmarks of surgical interest. These ligaments are fascial bands at specific sites, which serve to anchor the skin to the underlying bone. However, at websites the place retaining ligaments are present, the impact of gravitational pull is resisted. When performing facelift procedures, these ligaments should be surgically divided in order to facilitate redraping of facial pores and skin. Fascial areas Two tissue areas on the face could also be involved within the unfold of odon togenic infection. They are the buccal tissue area, lying between the skin and the surface of buccinator, and the infraorbital tissue space, mendacity between the bony attachments of levator labii superioris and levator anguli oris. The bones of the nasoethmoidal and zygomaticomaxil lary complexes are described here. The external floor is convex and clean, with a central parietal tuber (tuberosity).
Purchase procyclidine american express
Its upper 15 cm treatment juvenile arthritis discount 5mg procyclidine with amex, the filum terminale internum medicine advertisements buy procyclidine 5mg on line, is sustained within extensions of the dural and arachnoid meninges and reaches the caudal border of the second sacral vertebra medications multiple sclerosis order generic procyclidine canada. Its final 5 cm medicine in spanish buy procyclidine with amex, the filum terminale externum, fuses with the investing dura mater, after which descends to the dorsum of the first coccygeal vertebral section. A few strands of nerve fibres, which probably symbolize the roots of rudimentary second and third coccygeal spinal nerves, adhere to its upper part. They cross the subarachnoid space and traverse the dura mater individually, uniting in or close to their intervertebral foramina to form the (mixed) spinal nerves. Since the spinal cord is shorter than the vertebral column, the more caudal spinal roots descend for various distances around and beyond the wire to reach their corresponding foramina. In so doing, they type a divergent sheaf of spinal nerve roots, the cauda equina, which is gathered round the filum terminale in the spinal theca, principally distal to the apex of the cord. Note the fusiform cervical and lumbar enlargements of the cord, and the altering obliquity of the spinal nerve roots as the cord is descended. The cauda equina is undisturbed on the best however has been unfold out on the left to show its particular person elements. E, the lower end of the spinal cord, filum terminale and cauda equina uncovered from behind. F, A spinal twine phase displaying the mode of formation of a typical spinal nerve and the gross relationships of the grey and white matter. B�D, With permission from Waschke J, Paulsen F (eds), Sobotta Atlas of Human Anatomy, 15th ed, Elsevier, Urban & Fischer. Dorsal spinal roots bear ovoid swellings, the spinal ganglia, one on each root proximal to its junction with a corresponding ventral root in an intervertebral foramen. Each root fans out into 6�8 rootlets earlier than coming into the wire in a vertical row within the posterolateral sulcus. Dorsal roots are usually stated to comprise solely afferent axons (both somatic and visceral), that are the central processes of unipolar neurones in the spinal root ganglia, however they may also include a small quantity (3%) of efferent fibres and autonomic vasodilator fibres. Each ganglionic neurone has a single brief stem that divides into a medial (central) branch that enters the spinal twine through a dorsal root, and a lateral (peripheral) department that passes peripherally to a sensory end organ. The central branch is an axon whereas the peripheral one is an elongated dendrite (but when traversing a peripheral nerve is, in general structural phrases, indistinguishable from an axon). Distal to the foramen magnum, inside the vertebral column, the dura is distinct from the tissues that line the vertebral canal, and separated from them by the epidural area (see below). The spinal dura mater types a tube whose higher end is connected to the edge of the foramen magnum and to the posterior surfaces of the second and third cervical vertebral our bodies, and likewise by fibrous bands to the posterior longitudinal ligament, especially in the course of the caudal finish of the vertebral canal. It invests the thin spinal filum terminale, descends to the again of the coccyx, and blends with the periosteum. It is closed above by fusion of the spinal dura with the edge of the foramen magnum, and below by the posterior sacrococcygeal ligament that closes the sacral hiatus. It incorporates loosely packed connective tissue, fats, a venous plexus, small arterial branches, lymphatics and fine fibrous bands that join the theca with the liner tissue of the vertebral canal. These bands, the meningovertebral ligaments, are best developed anteriorly and laterally. There can be a midline attachment from the posterior spinal dura to the ligamentum nuchae at atlanto-occipital and atlantoaxial levels (Dean and Mitchell 2002). In the lumbar region, the dura mater is apposed to the walls of the vertebral canal anteriorly and attached by connective tissue in a way that allows displacement of the dural sac throughout movement and venous engorgement. Adipose tissue is current posteriorly in recesses between the ligamentum flavum and the dura. The connective tissue extends for a short distance via the intervertebral foramina along the sheaths of the spinal nerves. Like the principle thecal sac, the basis sheaths are partially tethered to the partitions of the foramina by fine meningovertebral ligaments. Local anaesthetics injected close to the spinal nerves, just outside the intervertebral foramina, could spread up or down the epidural house to affect the adjacent spinal nerves or might cross to the opposite side. The paravertebral spaces of Spinal twine and spinal nerves: gross anatomy A variety of pathological processes can happen within the epidural space, compressing the dura and leading to ache and potential neurological disturbance. For a review of the morphology of the epidural house and a dialogue of the character of the lining layer of the vertebral canal, see Newell (1999). The final of the dentate ligaments lies between the exiting twelfth thoracic and first lumbar spinal nerves and is a slim, oblique band that descends laterally from the conus medullaris. Changes within the form and position of the dentate ligaments throughout spinal movements have been demonstrated by cine-radiography. Beyond the conus medullaris, the pia mater continues as a coating of the filum terminale. Subdural space the subdural space is a potential area within the normal spine as a outcome of the arachnoid and dura are intently apposed (Haines et al 1993). Injection of fluid into the subdural area could damage the wire both by direct toxic effects or by compression of the vasculature. At websites where vessels and nerves enter or go away the subarachnoid area, the arachnoid mater is reflected on to the surface of those constructions and varieties a skinny coating of leptomeningeal cells over the surface of each vessels and nerves. Thus a subarachnoid angle is fashioned as nerves move via the dura into the intervertebral foramina. At this point, the layers of leptomeninges (arachnoid and pia) fuse and turn out to be steady with the perineurium. Dorsally, the intermediate layer is adherent to the deep side of the arachnoid mater and types a discontinuous sequence of dorsal ligaments that connect the spinal cord to the arachnoid. The dorsolateral ligaments are more delicate and fenestrated, they usually extend from the dorsal roots to the parietal arachnoid. As the intermediate layer spreads laterally over the dorsal surface of the dorsal roots, it turns into more and more perforated and finally disappears. A comparable arrangement is seen over the ventral aspect of the spinal cord however the intermediate layer is much less substantial. The intermediate layer is structurally just like the trabeculae that cross the cranial subarachnoid house, i. The ligamentum denticulatum is a flat, fibrous sheet on either aspect of the spinal wire between the ventral and dorsal spinal roots. These prolongations, the spinal nerve sheaths or root sheaths, progressively lengthen because the spinal roots become increasingly oblique. Each individual dorsal and ventral root runs within the subarachnoid space with its personal masking of pia mater. Each root pierces the dura individually, taking a sleeve of arachnoid with it, before becoming a member of within the dural prolongation simply distal to the spinal ganglion. The dural sheaths of the spinal nerves fuse with the epineurium, within or barely past the intervertebral foramina. At the cervical stage, where the nerves are brief and the vertebral motion is greatest, the dural sheaths are tethered to the periosteum of the adjoining transverse processes. The ventral, hypaxial, ramus is connected to a corresponding sympathetic ganglion by white and grey rami communicantes. It innervates the prevertebral muscular tissues and curves around within the physique wall to provide the lateral muscle tissue of the trunk. Near the mid-axillary line, it gives off a lateral department that pierces the muscular tissues and divides into anterior and posterior cutaneous branches. The major nerve advances in the body wall, where it provides the ventral muscles and terminates in branches to the pores and skin. Spinal nerves are united ventral and dorsal spinal roots, attached in collection to the edges of the spinal twine. The time period spinal nerve strictly applies solely to the brief phase after union of the roots and earlier than branching occurs. There are 31 pairs of spinal nerves: eight cervical, 12 thoracic, 5 lumbar, 5 sacral and 1 coccygeal. The nerves are numbered on the right aspect; the spines of the seventh cervical, sixth and twelfth thoracic, and first and fifth lumbar vertebrae are labelled on the left side. At thoracic, lumbar, sacral and coccygeal levels, the numbered nerve exits the vertebral canal by passing under the pedicle of the corresponding vertebra. However, in the cervical region, nerves Spinal nerves C1�7 pass above their corresponding vertebrae. C1 leaves the vertebral canal between the occipital bone and atlas, and hence is usually termed the suboccipital nerve.
Generic procyclidine 5mg amex
Mastoid half Zygomatic course of 624 the zygomatic course of juts forwards from the lower area of the squamous part treatment 1st degree burns generic procyclidine 5mg. The zygomatic process then twists anteromedially symptoms lung cancer purchase 5 mg procyclidine with mastercard, in order that its surfaces turn out to be medial and lateral treatment xerophthalmia buy 5mg procyclidine. The inferior floor is bounded by anterior and posterior roots treatment low blood pressure generic procyclidine 5 mg on line, converging into the anterior part of the method. The tubercle of the zygomatic root offers attachment to the lateral temporomandibular ligament at the junction of the roots. The posterior root is extended forwards above the exterior acoustic meatus, its upper border persevering with into the supramastoid crest. Very rarely, the squamous part is perforated above the posterior the mastoid half is the posterior area of the temporal bone and has an outer floor roughened by the attachments of the occipital stomach of occipitofrontalis and auricularis posterior. A mastoid foramen, of variable dimension and place, and traversed by a vein from the sigmoid sinus and a small dural department of the occipital artery, regularly lies near its posterior border. The foramen may be within the occipital or occipitotemporal suture; it might generally be parasutural or could additionally be absent. The mastoid part projects down because the conical mastoid course of and is larger in grownup males. Sternocleidomastoid, splenius capitis and longissimus capitis are all connected to its lateral surface, and the posterior belly of digastric is hooked up to a deep mastoid notch on its medial facet. The occipital artery runs in a shallow occipital groove that lies medial to the mastoid notch. The inside surface of the mastoid course of bears a deep, curved sigmoid sulcus for the sigmoid venous sinus; the sulcus is separated from the underlying innermost mastoid air cells by a skinny lamina of bone. The posterior border can be serrated and articulates with the inferior border of the occipital bone between its lateral angle and jugular process. The mastoid element is fused with the descending process of the squamous half; beneath, it seems within the posterior wall of the tympanic cavity. The posterior border, intermediate in size, bears a sulcus medially, which forms, along with the occipital bone, a gutter for the inferior petrosal sinus. Behind this, the jugular fossa contributes (together with the occipital bone) to the jugular foramen and is notched by the glossopharyngeal nerve. Bone on both or each side of the jugular notch may meet the occipital bone and divide the jugular foramen into two or three components. The anterior border is joined laterally to the squamous a part of the temporal bone at the petrosquamosal suture; medially, it articulates with the greater wing of the sphenoid bone. Two canals exist on the junction of the petrous and squamous elements, one above the opposite, separated by a skinny osseous plate and both leading to the tympanic cavity; the upper canal contains tensor tympani, while the decrease canal is the pharyngotympanic tube. It is inclined superiorly and anteromedially, and has a base, apex, three surfaces (anterior, posterior and inferior) and three borders (superior, posterior and anterior). The base would correspond to the part that lies on the base of the skull and is separated from the squamous half by a suture. The subsequent growth of the mastoid processes means that the exact boundaries of the base are no longer identifiable. The apex, blunt and irregular, is angled between the posterior border of the larger wing of the sphenoid and the basilar part of the occipital bone. It accommodates the anterior opening of the carotid canal and limits the foramen lacerum posterolaterally. Bone anterolateral to this impression roofs the anterior part of the carotid canal but is commonly deficient. A ridge separates the trigeminal impression from another hollow behind, which partly roofs the internal acoustic meatus and cochlea. Laterally, the anterior surface roofs the vestibule and, partly, the facial canal. Between the squamous part laterally and the arcuate eminence and the hollows just described medially, the anterior floor is shaped by the tegmen tympani, a thin plate of bone that forms the roof of the mastoid antrum, and extends forwards above the tympanic cavity and the canal for tensor tympani. The lateral margin of the tegmen tympani meets the squamous part at the petrosquamosal suture, turning down in entrance because the lateral wall of the canal for tensor tympani and the osseous part of the pharyngotympanic tube; its decrease edge is in the squamotympanic fissure. Anteriorly, the tegmen bears a narrow groove related to the larger petrosal nerve (which passes posterolaterally to enter the bone by a hiatus anterior to the arcuate eminence). The posterior slope of the arcuate eminence overlies the posterior and lateral semicircular canals. Lateral to the eminence, the posterior a half of the tegmen tympani roofs the mastoid antrum. The posterior floor contributes to the anterior a half of the posterior cranial fossa and is steady with the internal surface of the mastoid part. A small slit leading to the vestibular aqueduct lies behind the opening of the meatus, virtually hidden by a skinny plate of bone. This contains the saccus and ductus endolymphaticus, along with a small artery and vein. The terminal half of the saccus endolymphaticus protrudes by way of the slit between the periosteum and dura mater. Near the apex of the petrous half, a quadrilateral area is partly associated with the attachment of levator veli palatini and the cartilaginous pharyngotympanic tube, and partly related to the basilar a half of the occipital bone by dense fibrocartilage. Behind this area is the big, round opening of the carotid canal, and behind the opening of the canal is the jugular fossa, which is of variable depth and size, and accommodates the superior jugular bulb. The inferior ganglion of the glossopharyngeal nerve lies in a triangular despair anteromedial to the jugular fossa (below the internal acoustic meatus). At its apex is a small opening into the cochlear canaliculus, occupied by the perilymphatic duct (a tube of dura mater) and a vein draining from the cochlea to the internal jugular vein. A canaliculus for the tympanic nerve from the glossopharyngeal nerve lies on the ridge between the carotid canal and the jugular fossa. The mastoid canaliculus for the auricular branch of the vagus nerve is laterally positioned within the jugular fossa. Behind the jugular fossa, the rough quadrilateral jugular floor is covered by cartilage that joins it to the jugular process of the occipital bone. Tympanic half the tympanic a half of the temporal bone is a curved plate beneath the squamous part and anterior to the mastoid course of. Behind, it fuses with the squamous part and mastoid course of, and is the anterior limit of the tympanomastoid fissure. Its concave posterior surface forms the anterior wall, flooring and a part of the posterior wall of the exterior acoustic meatus. The tympanic membrane is hooked up to a slim tympanic sulcus on its medial surface. The quadrilateral concave anterior surface is the posterior wall of the mandibular fossa and may contact the parotid gland. Its tough lateral border varieties many of the margin of the osseous part of the external acoustic meatus and is continuous with its cartilaginous half. Laterally, the upper border is fused with the again of the postglenoid tubercle; medially, it types the posterior edge of the petrotympanic fissure. The inferior border is sharp and splits laterally to form, at its root, the sheath of the styloid process (vaginal process). The stylomastoid foramen lies between the styloid and mastoid processes; it represents the exterior end of the facial canal, contains a half of the aponeurosis of the posterior stomach of digastric, and transmits the facial nerve and stylomastoid artery. Often nearly straight, it could possibly show a curvature, an anteromedial concavity being most typical. Its proximal half (tympanohyal) is ensheathed by the tympanic plate, particularly anterolaterally, whereas muscular tissues and ligaments are hooked up to its distal half (stylohyal). The styloid course of is covered laterally by the parotid gland; the facial nerve crosses its base; the exterior carotid artery crosses its tip, embedded in the parotid; and medially, the method is separated from the start of the inner jugular vein by the attachment of stylopharyngeus. External acoustic meatus the temporal bone contains the bony (osseous) part of the external acoustic meatus. The squamous half is ossified in a sheet of condensed mesenchyme from a single centre near the zygomatic roots, which appears within the seventh or eighth week in utero. The petromastoid part has a quantity of centres that seem in the cartilaginous otic capsule in the course of the fifth month; as many as 14 have been described. Key: 1, helix; 2, crus of helix; three, auricular tubercle; 4, antihelix; 5, crura of antihelix; 6, triangular fossa; 7, scaphoid fossa; eight, concha of auricle; 9, exterior acoustic meatus; 10, tragus; eleven, antitragus; 12, intertragic notch; 13, lobule of auricle.