Cheap prothiaden 75 mg with visa
This work-up is crucial to assist information selections in regards to the appropriateness of implanting a device and the optimum medical technique during the endocardialization course of medications you cant crush buy 75 mg prothiaden overnight delivery. Because of a small incidence of atrial arrhythmias after system placement symptoms 8 days post 5 day transfer best prothiaden 75mg, a baseline electrocardiogram should also be obtained medications to treat bipolar disorder discount 75mg prothiaden free shipping. Procedural imaging consists of fluoroscopy with or with out echocardiography, most commonly intracardiac imaging. Quantification of a residual shunt by transcranial Doppler examination is useful to determine the need for repeated intervention. Normal ductal closure occurs throughout the first 12 hours after start by contraction and mobile migration of the medial smooth muscle within the wall of the ductus, leading to protrusion of the thickened intima into the lumen, inflicting useful closure. Final closure with creation of the ligamentum arteriosum is accomplished by three weeks of age; permanent sealing of the duct by infolding of the endothelium, disruption of the internal elastic lamina, and hemorrhage and necrosis in the subintimal region lead to alternative of muscle fibers with fibrosis. This strategy of closure is incomplete in 1 in 2000 reside births and accounts for as a lot as 10% of all congenital coronary heart illness. It is a particularly attractive technique in adults, in whom surgical ligation and division is usually a problem due to calcified ductal tissue and elevated surgical dangers. Several different closure devices are presently used due to the significant variability of ductal anatomy. For massive ducts, antegrade placement of an Amplatzer duct occluder device is the popular technique. In all however a very few sufferers, the coils may be snared from their embolized position in the pulmonary artery and faraway from the body with out sequela. Device embolization, thrombus, and ductal aneurysm have been reported in fewer than 1%. There have been no late reports of endocarditis after interventional closure of the ductus, though procedural infections have occurred hardly ever. Imaging Findings Preoperative Planning A full bodily examination and thoracic echocardiography are essential to make the analysis before intervention. Transthoracic echocardiography will present an abnormal systolic left-to-right color move jet into the primary pulmonary artery or proximal left pulmonary artery directed inferiorly and anteriorly. The central pulmonary arteries will be dilated, as will the left atrium and left ventricle if the shunt is important. Unusual variations of the ductus arteriosus include origin from the inferior side of the transverse arch and from the proximal innominate or subclavian artery. The anatomy of the ductus can range considerably; the most typical is conical, with the narrowing on the pulmonary artery finish. These various ductal anatomies can all be closed interventionally but require a selection of closure units. If pulmonary hypertension is famous during catheterization, an correct evaluation of the diploma of hypertension and the reactivity of the pulmonary bed have to be made throughout temporary occlusion of the ductus. Postoperative Surveillance nearly all of sufferers could be discharged on the identical day or the subsequent morning after the procedure. Predischarge analysis ought to embody a physical examination to assess for recurrence of ductal murmur (it could have disappeared with profitable closure) and sheath insertion web site. Uncommon but important issues related to ductal closure include proximal left pulmonary Outcomes and Complications Transcatheter ductal closure procedural success has been extremely excessive, with charges of full closure above 96%. If left pulmonary artery stenosis is confirmed on echocardiography, a nuclear medication pulmonary move scan should be obtained to consider the physiologic significance of the obstruction. Coarctation is most often a discrete narrowing of the proximal descending thoracic aorta simply distal to the origin of the left subclavian artery at the site of the ductus ligamentum. It represents 7% of all sufferers with congenital heart disease and results in higher extremity hypertension, left ventricular hypertrophy, and ultimately ventricular failure whether it is left untreated. It must be thought of through the initial evaluation of systemic hypertension and can simply be identified on physical examination by decreased femoral pulses with a delay in contrast with radial pulses and blood pressure differential between the arms and legs. The narrowing is because of thick intimal and medial ridges that protrude posteriorly and laterally into the aortic lumen. Cystic medial necrosis with disarray and lack of medial elastic tissue happens generally within the adjacent aorta and will lengthen to the ascending aorta as nicely. Enlargement of the intercostal arteries because of this collateral flow is the mechanism for rib notching seen on chest radiography in older sufferers with extreme native coarctation. Indications Any coarctation with a gradient of greater than 10 mm Hg and significant higher body hypertension or left ventricular hypertrophy without additional trigger must be handled. Mild coarctations with a gradient of less than 20 mm Hg without hypertension or left ventricular hypertrophy should be considered for stent restore if collaterals are present or the patient has an abnormal blood strain response to exercise. Stent implantation for repair of coarctation was performed sporadically within the early Nineties in youngsters; it was first reported in adults in 1995 with very promising results. Procedural success has been reported in additional than 95% of sufferers, with residual obstruction of lower than 20 mm Hg. Recurrent stenosis has been extraordinarily rare, occurring in fewer than 5%, often in younger sufferers, and is mostly gentle. Complications have been reported in up to 20% and embody aneurysm, perforation, stroke, and demise in fewer than 3%. Imaging Findings Preoperative Planning Echocardiography is helpful to confirm the prognosis and to consider location and severity of the obstruction. Special consideration must be paid to the surrounding aortic diameter, including the distal transverse arch, the coarctation diameter, and the placement relative to the carotid and left subclavian arteries, in addition to to the presence of existing aneurysm, poststenotic dilation, and calcification. Final evaluation of the coarctation is performed through the procedure with biplane angiography, including during and after balloon dilation or stent implantation. Patients with mild coarctation (<20 mm Hg) without higher physique hypertension ought to have blood pressure checks every 6 to 12 months with ongoing surveillance for the event of left ventricular hypertrophy. Patients with vital hypoplasia and obstruction of the transverse aortic arch within the space of the origin of the carotids ought to be excluded. Stent restore with jailing of the carotids may be appropriate within the uncommon patient at extremely excessive surgical risk; nevertheless, for the majority of patients with this lesion, surgical repair must be performed. Covered thoracic stents might have a role in this setting, though there are restricted data at present. Aortic wall dissection, aneurysm, and rupture related to stent implantation are uncommon but improve in frequency with the age of the affected person and the diploma of aortic calcification related to the coarctation. Postoperative Surveillance Most sufferers are discharged on the day after the implantation or dilation, and chest radiography should be performed earlier than discharge to guarantee steady stent placement. Because late aneurysms might happen in up to 7% as late as 10 years, ongoing imaging surveillance is required. Normal distribution of pulmonary circulate is 55% to the proper lung and 45% to the left lung. Patients with a reduction of more than 15% of move or an absolute flow of less than 1 L/min/m2 in the affected lung ought to be thought of for stent restore. Patients with any diploma of contralateral pulmonary artery hypertension, proper ventricular hypertension, or right ventricular hypertrophy ought to be aggressively treated to prevent development, as ought to patients with important pulmonary insufficiency associated with the branch pulmonary artery stenosis. Contraindications Adult sufferers after restore of complicated congenital heart disease similar to tetralogy of Fallot or truncus arteriosus are complex, often with multiple anatomic, hemodynamic, and arrhythmia issues along with their branch pulmonary artery stenosis. It is critical that these patients are evaluated utterly and that a comprehensive plan is made in coordination with a heart specialist familiar with congenital coronary heart disease and involving an electrophysiologist, cardiothoracic surgeon, and interventionalist. If surgical revision of the underlying restore is required, a surgical strategy to the department pulmonary artery stenosis may be preferable. Outcomes and Complications Balloon dilation of branch pulmonary artery stenosis was initially described in 1983 by Lock and colleagues27; nonetheless, solely 50% of lesions responded, with a big restenosis fee. With the availability of larger peripheral stents in the early Nineties and their software to pulmonary artery department stenosis,28 stent placement has quickly turn into the treatment of selection in school-age kids and adults due to improved success and low restenosis rates. Shaffer and coworkers29 reported leads to greater than a hundred thirty youngsters and adults with postoperative department pulmonary artery stenosis; in more than 65%, stent implantation increased lesion diameter by more than 100%, with a median gradient discount from forty six to 10 mm Hg and right ventricle�to�systemic pressure ratio discount from 60% to 40%. Complications are uncommon, occurring in fewer than 4% of circumstances total, and embody hemoptysis, aneurysm, perforation, refractory ventilation-perfusion mismatch, and dying. Technical points, corresponding to system malposition and embolization, have been reported in less than 2% and are fairly rare with current enhancements in balloon and stent know-how. Recent use of slicing balloons has additional improved results to greater than 90% success for segmental pulmonary artery stenosis resistant to normal dilation and stenting methods. Branch pulmonary artery stenosis is a rare congenital lesion in isolation but is commonly related to advanced congenital heart lesions after surgical restore, especially tetralogy of Fallot. Other associated lesions embody truncus arteriosus or pulmonary atresia with ventricular septal defect after right ventricle�to�pulmonary artery conduit placement, transposition of the good arteries after arterial switch restore, and pulmonary artery sling after reimplantation.
Diseases
- Lysosomal alpha-D-mannosidase deficiency
- Chaotic atrial tachycardia
- Follicular hamartoma alopecia cystic fibrosis
- Schindler disease
- Essential mixed cryoglobulinemia
- Uhl anomaly
- Syndactyly type 3
- Vestibulocochlear dysfunction progressive familial
- Wells syndrome
- Short limb dwarf lethal Colavita Kozlowski type
Discount 75mg prothiaden with visa
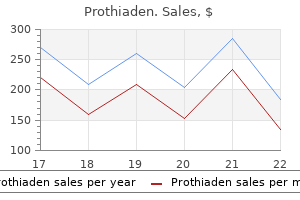
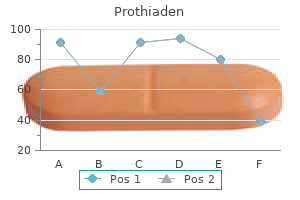
End-diastolic (left) and end-systolic (middle) volumes present severe international hypokinesis in all regions treatment action group discount prothiaden 75mg without a prescription. Volume curves (right) present irregular left ventricular end-diastolic and end-systolic volumes medicine for runny nose purchase 75mg prothiaden, and irregular left ventricular ejection fraction of 16% xerostomia medications side effects discount 75 mg prothiaden free shipping. If the chest ache has resolved at the time of radiotracer administration, take a look at sensitivity is modestly decreased, and present guidelines suggest repeating radiotracer administration inside 2 hours of symptom abatement. The adverse predictive worth of a normal or mildly abnormal research can also be very excessive; these sufferers have a cardiac mortality of lower than 1% per year, which is roughly the same as that of the final population. A highly irregular study with severe and in depth perfusion abnormalities can have a cardiac occasion fee of 6% to 8% per 12 months. As previously mentioned, an necessary specific indication is for the analysis of myocardial viability. Inferoseptal area (small yellow arrows), at the periphery of the infarct, shows partial enchancment (compare stress with relaxation images). Contraindications for pharmacologic stress testing are related to the particular pharmacologic stress brokers administered, and are described in the next section underneath pharmacologic stress testing. These phantoms have solid "cold" spheres of differing sizes, and are full of background radioactivity. The phantom assesses threedimensional spatial resolution, uniformity, and tomographic picture contrast. We suggest abstinence from caffeinated substances due to the possibility that a pharmacologic stress check could additionally be needed if an insufficient maximal coronary heart fee is reached during maximal train stress testing. Patients with good functional capacity can typically exercise on the Bruce protocol, which rapidly will increase in velocity and incline. A2A is taken into account a cardiac specific receptor, by way of which coronary vasodilation is initiated after intravenous adenosine administration. Adenosine causes a vasodilation without direct chronotropic or inotropic responses in myocardium. Secondary hemodynamic changes in response to vasodilation embody a modest lower in systolic and diastolic blood strain, and a compensatory improve in heart rate with modest improve in cardiac output. Adenosine has a really quick half lifetime of 10 to 15 seconds and is administered at the fee of one hundred forty �g/kg/min over four minutes. The stress radiotracer is administered after four minutes of infusion to outline coronary blood flow at maximal vasodilation. Side results are just like dipyridamole, but additionally embody atrioventricular block. The most typical unwanted facet effects are intermittent Description of Techniques and Protocols Radionuclide Imaging Protocols Stress Protocols-Pharmacologic versus Exercise Protocols the commonest kinds of stress protocols within the United States are train treadmill and pharmacologic stress check. Additionally, train typically leads to decrease radiotracer uptake within the gastrointestinal tract, improving image high quality. The pharmacologic brokers routinely utilized in clinical apply are adenosine, dipyridamole, and dobutamine. Patients with left bundle branch block, a recognized explanation for false-positive septal perfusion defects with train, might undergo stress testing carried out with dipyridamole to lower the potential for this artifact. Other limiting components in train stress testing are bodily deconditioning, peripheral vascular disease, historical past of stroke, lower extremity amputation, and severe chronic obstructive pulmonary disease. Exercise Protocols In normal people, peak exercise increases heart rate and myocardial oxygen demand. Because of the very quick physiologic half-life, these side effects are very short-lived and resolve within 1 to 2 minutes of discontinuation. This leads to a excessive local interstitial concentration, which subsequently ends in coronary vasodilation. The commonest unwanted effects include headache, flushing, hypotension, nausea, and chest discomfort. Because of a relatively longer biologic half-life of dipyridamole, the radiotracer is run at 6 minutes after the start of the dipyridamole infusion. In addition, unwanted facet effects may last for several minutes, however may be rapidly reversed by intravenous infusion of aminophylline, which acts by competitively inhibiting adenosine binding to its receptors. Compared with adenosine, dipyridamole is equally effective in producing coronary vasodilation, and has a decrease total incidence of unwanted effects, including induction of atrioventricular block. Dipyridamole can be utilized in patients with prolonged P�R interval and in aged sufferers with poor tolerance to unwanted aspect effects. Severe hypotension, ventricular tachycardia and hemodynamically unstable sustained supraventricular tachycardia, and atrial fibrillation with speedy ventricular response are indications for termination of dobutamine. Other side effects of dobutamine embody chest ache, dyspnea, palpitations, hypertension, nervousness, nausea, and vomiting. Contraindications to dobutamine embrace ventricular tachycardia, atrial fibrillation with rapid ventricular response, uncontrolled hypertension, hypotension, hypertrophic obstructive cardiomyopathy or aortic stenosis with extreme left ventricular outflow obstruction, latest aortic dissection, and coronary artery dissection. Although modest differences exist, general accuracy of the commonest protocols is comparable. When utilizing same-day protocols with Tc 99m radiotracers, however, the resting study must be performed first to keep away from "false-positive" fastened defects. If the resting research is performed first, the following stress exercise is far higher (approximately thrice higher), and the increased blood move at stress (approximately 2. The number of potential false-negative outcomes for ischemia is small as a end result of the resting activity has a comparatively small contribution to the stress imaging. Contraindications to Vasodilator Stress Testing Vasodilators are contraindicated in patients with extreme continual obstructive pulmonary illness and asthma, notably patients presently receiving therapy with -agonists. Because excessive levels of adenosine block the -agonist activity of bronchodilators, sufferers with chronic or reactive airways illness may experience bronchoconstriction and respiratory compromise. Unstable angina, persistent hypotension with systolic blood stress less than 90 mm Hg, high-grade atrioventricular block without a pacemaker, uncontrolled arrhythmias, and severe aortic stenosis are additionally contraindications. Because xanthines block adenosine receptors, these must be discontinued at least 24 hours before vasodilator stress testing. Acquisition Protocols the following protocols are suggested pointers for an average-sized 70-kg man. For larger sufferers, rising administered exercise, imaging time, or both could partially compensate for the loss in detected true counts and subsequent lower in image high quality. Generally, the multiheaded gamma digicam parameters for acquisition are similar for thallium 201 and Tc 99m radiotracers. This can be carried out routinely with out adversely rising imaging time or Pharmacologic Protocols-Dobutamine Dobutamine is a -adrenergic agent with a biologic halflife of two minutes. It acts by rising myocardial contraction and heart price, which subsequently increases myocardial oxygen demand and blood flow. Intravenous administration starts at an preliminary dose of 5 to 10 �g/kg/min for 3 minutes, with subsequent will increase to doses of 20 �g/kg/min, 30 �g/kg/min, and 40 �g/kg/min in 3-minute phases, or until the aim of reaching 85% of maximal heart price goal is achieved. The gated photographs are reconstructed and displayed in cine format for evaluation as described subsequently. A limitation of this system is the requirement of a comparatively common rhythm over the imaging interval. Stress imaging begins approximately 15 minutes to 1 hour after the stress injection of 1. The time interval between radiotracer administration and the beginning of imaging varies. Delayed imaging may favor improved liver clearance; nevertheless, earlier imaging might reduce bowel exercise. An advantage of this protocol is the short time interval between the initial resting injection and the stress study. The major disadvantage of this protocol pertains to differences in last picture high quality. Thallium 201 has a decrease photopeak vitality, for which gamma cameras have inferior power resolution and spatial decision compared with greater gamma ray energies. The lower thallium 201 photographs additionally contain a larger proportion of Comptonscattered gamma rays than do photographs acquired at greater energies. These factors, combined with decrease administered exercise at decrease resting blood flow, all contribute to general lower true counts and the need for greater diploma of filtering. Care is taken specifically to process these completely different radiotracer studies with specific protocols.
Purchase genuine prothiaden
Identification of such abnormalities is often critical to planning of reintervention or medical management medications rapid atrial fibrillation purchase 75 mg prothiaden with amex. Not only is that this population of sufferers growing older sufficiently to develop atherosclerotic coronary artery illness medications j-tube order 75mg prothiaden with mastercard, in addition they commonly have congenitally abnormal or postoperatively acquired coronary artery lesions treatment quinsy purchase genuine prothiaden on line. This malformation consists of 1 embryologic abnormality, namely, anterior malalignment of the infundibular septum, leading to 4 fixed options: malalignment ventricular septal defect, subvalvular (infundibular) and valvular pulmonary stenosis, overriding aorta, and proper ventricular hypertrophy. Early repair in the first few months of life is now possible and recommended as normal of care. The objectives of definitive restore are to shut the ventricular septal defect and to relieve right ventricular outflow tract obstruction (placement of a right ventricle�to�pulmonary artery conduit in sufferers with pulmonary atresia, placement of a transannular patch in these with severe pulmonary stenosis, or infundibular muscle resection in these with delicate pulmonary stenosis). In addition, progressive right ventricular dilation typically leads to tricuspid valve annular stretch and in the end regurgitation, which perpetuates continued proper ventricular dilation. A two-dimensional airplane is chosen throughout the principle pulmonary artery for quantification of right ventricular stroke quantity and pulmonary regurgitation (as a net quantity in addition to a share of the stroke quantity; see. In addition, a two-dimensional plane may be prescribed in the airplane of the right ventricular outflow tract to acquire a peak velocity and to quantify a peak stress gradient if echocardiographic evaluation proved insufficient. A baseline study ought to be obtained in late childhood when sedation now not is critical. This circulation is typically not suitable with life except surgical procedure is performed to redirect deoxygenated circulate to the lungs and oxygenated circulate to the physique. Until the mid-1980s, this defect was surgically corrected with an atrial-level change (Senning or Mustard procedure). The arterial change (Jatene procedure) turned well-liked within the mid-1980s and remains the usual of care in this population of patients. Right ventricular dilation and failure are often accompanied by tricuspid (systemic atrioventricular valve) regurgitation, which results in worsening right ventricular dilation and dysfunction. Axial plane and coronal indirect planes via the superior vena cava and inferior vena cava pathways are useful for diagnosis of obstruction to flow. In addition, the coronary artery ostia and proximal coronary arteries could be evaluated. Patients with native or repaired coarctation of the aorta typically suffer aortic complications, corresponding to restenosis, aneurysm formation of the ascending aorta or repair website, dissection, systemic hypertension with left ventricular hypertrophy, and early coronary artery illness. The circulate curves demonstrate the move in the ascending aorta (B) and descending aorta (C). The delayed onset of systolic move, damped price of return to baseline, and chronic flow throughout diastole seen within the descending aorta are suggestive of serious obstruction. This contains anatomic characterization of recurrent or residual obstruction, relationship of the obstruction to different arch vessels (which is critical for planning of surgical or catheter-based interventions), arch anatomy. The second objective is to consider the impact of the obstruction or resultant systemic hypertension on the myocardium, including left ventricular myocardial mass and left ventricular perform. The last aim is to confirm the physiologic severity of the obstruction by evaluating the nature of move on the obstruction and within the descending aorta. It is from these images that cross-sectional areas can be measured, arch anatomy may be delineated, and collaterals can be defined. These findings are crucial to planning of medical, catheter-based, or surgical interventions. First, a twodimensional plane across the cross-sectional area of the ascending aorta is obtained. If prescribed nicely, this often yields not only move within the ascending aorta but additionally flow in the descending aorta just distal to the obstruction. It is also useful to acquire move in the descending aorta at the level of the diaphragm. Delayed onset of systolic circulate, damped price of return to baseline, persistent flow during diastole, and augmentation of circulate secondary to collaterals are suggestive of significant obstruction. Sagittal indirect plane within the long axis of the aorta ought to be obtained, the so-called candy cane view. They often have single proper ventricles that ultimately fail within the face of systemic afterload. They might have valvular illness that will increase the stress or volume load of the only ventricle. The second objective is the characterization of physiology, including valvular disease, myocardial perform, and circulate evaluation. Both the area of coarctation of the aorta and the collaterals are recognized (arrows). In the current era, they usually endure several surgical procedures in the course of the first several years of life to provide a stable cardiopulmonary physiology. The first of these procedures is usually performed in the neonatal period and is directed at recruiting the single ventricle because the systemic pumping chamber and offering controlled pulmonary blood move. The subsequent procedures involve sequential conversion to a physiology of separated systemic and pulmonary circulations with passive pulmonary blood flow (elimination of intracardiac "mixing"). The final circulation is identified as the Fontan circulation after the French surgeon who developed and first carried out it in humans. Images ought to extend from the diaphragm to the arch vessels to start to assess cardiac and vascular anatomy. Black blood imaging may be helpful if anatomy is in query or if there are metallic devices in place inflicting artifact on cine imaging. First, two-dimensional planes are prescribed across the aorta as well as the vessels supplying blood move to the pulmonary vascular bed. Twodimensional flow evaluation throughout the atrioventricular valves as properly as the superior and inferior venae cavae is often helpful for assessment of atrioventricular valve regurgitation and for corroboration of other flow and volumetric data. A seven-dimensional flow method could prove helpful on this anatomy and physiology as it could possibly acquire move in all vessels in a single acquisition. First, because of the passive nature of pulmonary blood flow, they develop excessive right-sided filling pressures, dilated Fontan pathways, and atrial arrhythmias. As a result of high filling pressures, they typically type systemic-to-pulmonary venous collaterals, which result in cyanosis. Serial examinations ought to be carried out, the frequency of which must be dictated by medical standing. Clinical applications of cardiovascular magnetic resonance in congenital heart disease. Thoracic cardiovascular anomalies in children: evaluation with a quick gradient-recalledecho sequence with cardiac-triggered segmented acquisition. Comparison of gated single-photon emission computed tomography with magnetic resonance imaging for evaluation of left ventricular perform in ischemic cardiomyopathy. The vary of regular values of cardiovascular buildings in infants, children, and adolescents measured by magnetic resonance imaging. Delayed-enhancement cardiovascular magnetic resonance identifies fibrous tissue in children after surgical procedure for congenital heart disease. Magnetic resonance imaging analysis of myocardial perfusion and viability in congenital and acquired pediatric heart disease. Free-breathing, three-dimensional coronary artery magnetic resonance angiography: comparison of sequences. Diagnostic efficiency of coronary magnetic resonance angiography as in contrast against conventional x-ray angiography: a meta-analysis. Effect of chronic sustainedrelease dipyridamole on myocardial blood circulate and left ventricular perform in sufferers with ischemic cardiomyopathy. Prognostic value of cardiac magnetic resonance stress tests: adenosine stress perfusion and dobutamine stress wall movement imaging. Prognosis of negative adenosine stress magnetic resonance in sufferers presenting to an 30. White Imaging of coronary atherosclerosis has relied on coronary angiography as the gold normal since Sones and Shirey developed the technique at the Cleveland Clinic within the Sixties. Although the in vivo demonstration of vulnerable plaques, allowing for prevention of plaque development, is yet elusive, it might be only a matter of time earlier than coronary angiography is replaced by noninvasive strategies as the first device for coronary atherosclerotic imaging. The prevalence is affected by age, gender, genetic predisposition, and purchased danger factors.
Generic prothiaden 75mg without prescription
The prevalences of these entities are tough to discern as aneurysms have broad variations in definition and the opposite aortic manifestations are under-reported treatment with chemicals or drugs prothiaden 75 mg for sale. Atherosclerosis growth represents much more than simply accumulation of lipid symptoms 5 weeks pregnant cramps purchase prothiaden 75mg visa. It stems from a collection of advanced cellular and molecular processes that are initiated because of the various known atherosclerotic threat components and comorbid circumstances that cause the preliminary levels of atherosclerosis to progress in a predictable style symptoms vaginal cancer order prothiaden on line. The pathophysiologic means of atherosclerosis stays predominantly uniform across the spectrum of affected arterial beds, though there are some key regional variations. Atherosclerosis is a illness primarily of the massive and medium-sized arteries and is more and more thought-about primarily an inflammatory process in response to endothelial injury and lipid oxidation. Positive suggestions leads to repeated cycles of this process, and progressive arterial dilation (Glagov phenomenon) and ultimately luminal encroachment occur. Alternatively, rupture of the fibrous cap can occur, leading to rapid platelet aggregation, thrombosis, fast vessel obstruction, and medical occasions. Several hypothetical frameworks have been developed to help explain this advanced process. These lipid-laden macrophages are known as foam cells because of their histologic appearance. Extracellular Matrix Formation and the Fibrous Cap Progressive irritation results in activation of the infiltrating T lymphocytes and macrophages. These then secrete a variety of cytokines, chemokines, lytic enzymes, and development elements that stimulate the formation of an extracellular matrix. Continued development of this matrix induces the creation of a fibrous cap over the proliferating easy muscle cells and necrotic lipid core. Progression to Clinical Significance During the initial phases of atherosclerosis, the blood vessel dilates to keep lumen size, a process known as the Glagov phenomenon. However, the repeated cycles of irritation, clean muscle cell and fibrous tissue proliferation, and growth of the lipid core eventually overwhelm the compensatory response, resulting in progressive luminal obstruction. Decreased luminal blood flow from the growing vessel blockage will finally result in inadequate provide to meet oxygen demand, and ischemia will ensue. More fast vessel occlusion also can happen, leading to ischemia and potentially infarction, depending on the vascular bed. The activated T lymphocytes present can secrete matrix metalloproteinases and different lytic molecules that may degrade the fibrous cap, leading to cap rupture and the uncovering of the prothrombotic elements beneath. They additionally result in inflammatory cell and platelet adhesion, amplified endothelial permeability, clean muscle cell proliferation, and lack of exercise of vasodilatory and fibrinolytic brokers similar to nitric oxide, inflicting increased endothelial procoagulancy. Endothelial harm also leads to platelet deposition and resultant monocytic and T-cell infiltration. Cumulatively, these factors result in increased oxidative stress, which facilitates the following step in the atherosclerotic course of. The artery on the left has early atherosclerotic findings, together with a small lipid core. As the atherosclerosis progresses, the lipid core enlarges, but the artery dilates eccentrically to preserve the original lumen size. Eventually, the lesion development is enough to overload the compensatory dilation, and lumen encroachment occurs (not shown). Reactive oxygen species induce necrosis and apoptosis, leading to a necrotic core. Inflammatory cells promote cytokine and development issue release that stimulates fibrous cap formation. Risk Factors the danger elements for atherosclerosis are similar throughout the a number of arterial beds affected, whatever the end-organ perfused. They fall into two categories: those which are modifiable and those past our management. Modifiable danger elements may be further broken down into those that are predominantly a results of lifestyle indiscretions and those that are primarily manifestations of scientific illness that can be treated (Table 88-1). The atherosclerotic course of occurs in a stepwise trend over time, and people with superior age usually have a tendency to have a higher burden and larger complexity of illness. Data from the Framingham research show that 7% to 9% of people seventy five years of age or older have carotid stenoses of 50% or extra. However, with the rising variety of female people who smoke and disproportionate prevalence and rate of enhance in obesity, these gender differences are narrowing. For occasion, black populations have a 38% greater incidence than do white populations of ischemic stroke and stroke mortality adjusted for risk elements. This is obvious from research of common carotid artery wall thickness and abdominal calcification, during which familial factors contribute 64% to 92% and 50% of the variation, respectively. The majority of isolated riskassociated genes to date modulate other recognized cardiovascular danger elements quite than the atherosclerotic process itself. Genes that work independently of recognized comorbid conditions are the topic of intense ongoing research. The proposed mediators of this increased risk embrace immune complicated deposition; elevated fibrinogen, von Willebrand issue, and other procoagulants; higher lipoprotein ranges from glucocorticoid therapy; and direct vascular injury with endothelial cell progenitor cell depletion. Modifiable Risk Factors Many of the known modifiable threat components have wellestablished interactions with the pathophysiologic processes of noncoronary atherosclerosis. The black inhabitants has the next rate of atherosclerosis than the white population does. Smoking Diabetes Hypertension Hypercholesterolemia Hyperhomocysteinemia C-reactive protein zero. Lipoxygenase additionally will increase free radical production and subsequently reduces nitric oxide formation. Homocysteine decreases nitric oxide availability in addition to its direct toxicity to the endothelium and its prothrombotic effects. The Edinburgh Artery Study particularly addressed the differential odds ratios by measuring danger elements and analyzing the prevalence of these two situations in 1592 subjects both with and without a history of tobacco use. Increased levels of C-reactive protein promote apoptosis and stimulate procoagulant tissue factors, leukocyte adhesion molecules, and inhibitors of fibrinolysis. The hyperglycemia, insulin resistance, and fatty acid manufacturing associated with diabetes cut back the bioavailability of nitric oxide, decreasing vasodilation and permitting elevated easy muscle cell proliferation and platelet activation. Finally, diabetes increases procoagulant tissue factor and fibrinogen manufacturing, leading to a hypercoagulable state. Triglyceride-rich lipoproteins stimulate smooth muscle cell proliferation and extracellular matrix deposition. This threat factor complex leads to a low-grade inflammatory state with increased ranges of C-reactive protein, tumor necrosis factor, and fibrinogen. Moreover, every part of the metabolic syndrome independently increases atherosclerotic risk. Adipose tissue worsens insulin sensitivity and causes a system-wide proinflammatory state. Persistent hyperglycemia from insulin resistance and the high coprevalence of diabetes mellitus lead to advanced glycation end-products that trigger extra arterial inflammation. Both bodily inactivity and obesity have been proven to enhance C-reactive protein levels and to trigger endothelial dysfunction. They also worsen many other illness states that independently increase the chance of illness. However, novel contributors of risk, particularly those estimating inflammation, similar to high-sensitivity C-reactive protein, lipoprotein(a), and homocysteine, are difficult these present paradigms. These novel elements may have additional predictive worth only in sufferers with untimely or quickly progressive disease. There is some variation in threat factors primarily based on the anatomic localization of illness. For instance, in aortic illness, tobacco use continues to play a significant role (partly because of elastin degradation). Other than these examples, few information are available on gender- and ethnicity-based risk differences. This consists of all patients older than 70 years, these aged 50 years or older with diabetes or a history of tobacco use, and youthful sufferers with diabetes and any further atherosclerotic threat components. Classic intermittent claudication involves leg fatigue or discomfort, usually in the calf, that occurs only with exertion and is relieved after not extra than 10 minutes of relaxation. This makes a cautious physical examination and targeted noninvasive imaging even more necessary. An essential part of a basic evaluation of systems is a historical past of aortic aneurysmal disease in a first-degree relative. Mesenteric arterial disease is poorly studied due to its vague scientific presentation but carries a very poor prognosis and is usually related to different atherosclerotic illness.
Vitamin A. Prothiaden.
- Improving recovery from laser eye surgery when used in combination with vitamin E.
- How does Vitamin A work?
- Reducing problems during pregnancy and after giving birth in underfed (malnourished) women.
- Dosing considerations for Vitamin A.
- Breast cancer.
- Reducing complications of diseases such as malaria, HIV, measles, and diarrhea in children with vitamin A deficiency.
- What is Vitamin A?
- Anemia.
- Reducing fetal and early infant death in children born to women with nutrition problems.
- Prevention of cataracts.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96926
Buy prothiaden paypal
Digital subtraction angiography could additionally be a helpful adjunct for preoperative planning before carotid subclavian bypass medications that cause constipation purchase generic prothiaden pills. Angiography can determine main inflow and outflow vessels in addition to necessary collaterals medicine 0636 purchase discount prothiaden line. Postoperative Surveillance the location of the bypass graft within the neck makes duplex ultrasonography the modality of selection for postoperative graft surveillance medicine cups cheap 75 mg prothiaden with amex. Duplex ultrasonography can identify lesions of the proximal and distal anastomoses along with modifications of velocities inside the graft. Once a threatened bypass has been identified with duplex ultrasonography, angiography may be used to further examine the anastomoses and to delineate intragraft stenoses. Intraoperative administration of patients with thoracoabdominal aneurysms relies on the extent of the aneurysmal degeneration of the aorta. In the thorax, the recurrent laryngeal and vagus nerves are gently retracted off from the aorta. All large intercostal arteries from T7 to L2 are reimplanted into the graft, followed by the visceral vessels. If stenoses at the origin of those arteries are encountered, an endarterectomy could additionally be performed. Finally, the distal anastomosis is carried out in endoaneurysmal style to an uninvolved portion of the distal aorta. Finally, aneurysms producing distal embolization may be considered for restore regardless of measurement. Chest radiography may reveal aortic dilation within the presence of calcification, however the films are regularly regular. These sufferers are usually recognized on preoperative cardiac stress testing as nicely as on preoperative pulmonary function testing. Relative contraindications embrace decreased life expectancy associated to different medical points. The patient underwent open debranching of the celiac, superior mesenteric, and bilateral renal arteries with a branched graft from the distal aorta (C and D, small arrow). A distal aorto�left femoral graft was also placed that was used for entry within the subsequent endovascular repair (C and D, large arrow). Indications Endovascular repair of thoracic aneurysms may be restricted by gadget sheath diameter that exceeds the diameter of the access arteries or heavy calcification and tortuosity of the access arteries. In the case of distal open entry, an aortofemoral bypass could also be performed either alone or in conjunction with concomitant debranching or repair of an aortic aneurysm. Anatomic requirements include 20 mm or more of proximal and distal neck length and distal neck diameters of 20 to forty two mm. A four-limbed bypass was anastomosed to the ascending aorta for device entry as nicely as for debranching of the arch vessels (B). In the perioperative interval, 10% of patients require reintervention; freedom from reintervention approaches 81% by forty eight months. The perioperative mortality rate is approximately 10% and is half that of an open restore. With either process, proximal and distal control of the aorta and iliac arteries is obtained. In the case of juxtarenal and suprarenal aneurysms, a supraceliac clamp must be positioned. An infrarenal artery clamp is positioned simply distal to the left renal vein within the case of an infrarenal aneurysm. If a supraceliac clamp is in place, the renal arteries are sometimes flushed with iced heparinized saline to stop ischemic damage. The visceral vessels could also be reimplanted on the graft if that portion of the aorta is aneurysmal. The proximal clamp is then eliminated and positioned on the proximal graft, reestablishing blood flow to the kidneys within the case of supraceliac clamping. The inferior mesenteric artery, if patent, could additionally be ligated within the presence of strong backbleeding or reimplanted within the presence of poor backbleeding. Finally, the aneurysm sac is closed over the graft to prevent contact with and probably erosion into surrounding structures postoperatively. Emergent upper endoscopy for affirmation of the diagnosis, followed by extra-anatomic bypass and resection of the graft, is warranted. Operative risk is elevated in sufferers with chronic renal insufficiency, chronic obstructive pulmonary illness, congestive heart failure, average to extreme coronary artery illness, and superior age. Imaging Findings Preoperative Assessment Ultrasonography is the first modality for the identification of abdominal aortic aneurysmal illness because of its low value and ease of detection. Not only does it present a extra accurate diameter measurement than ultrasonography, however it assesses the whole aorta for pathologic changes. This turns into clinically relevant past 3 mm of dilation and is seen in roughly 13% of patients. The affected person underwent open aneurysm restore with ligation of the distal left common iliac artery, endarterectomy of the proximal left exterior iliac artery because of heavy calcification precluding standard anastomosis, and femoral anastomosis of the left graft limb. B, Postoperative picture shows the aneurysm repair with retrograde circulate through the left exterior iliac artery into the left inside iliac artery. The affected person was discovered to have expansion of the internal iliac artery aneurysms (large arrows) because of retrograde move from pelvic collateral circulation. End-to-side proximal anastomoses preserve pelvic blood circulate; end-to-end proximal anastomoses could additionally be most popular to maximize blood move to the lower extremities in sufferers with complete occlusion of the aorta and inner iliac arteries. Once the proximal anastomosis is full, the limbs of the bifurcated graft are tunneled just anterior to the native widespread and exterior iliac arteries, posterior to the ureters, after which under the inguinal ligament. Hybrid restore is helpful in these situations to avoid the morbidity of an open repair. In these situations, an aortorenal or iliorenal bypass could additionally be needed earlier than the position of the endograft. Contraindications Aortobifemoral bypass is associated with important cardiopulmonary morbidity. A bypass from the right exterior iliac artery to the accessory right renal and inferior mesenteric arteries was carried out before endografting to preserve blood flow to the best kidney and pelvis. The aneurysm was then repaired with a standard endograft whose distal limbs covered each inner iliac arteries. Such sufferers are better served with extra-anatomic bypass despite the decreased patency charges of those procedures. Outcomes and Complications Outcomes of aortobifemoral bypass are glorious, with 5-year patency charges starting from 85% to 95%. Complications occur sometimes and are sometimes cardiopulmonary and renal in nature. One unique complication related to this process is the event of thigh and buttock claudication in as much as 30% of patients present process aortobifemoral bypass. Imaging Findings Preoperative Assessment Preoperative assessment of sufferers with aortoiliac occlusive illness begins with noninvasive vascular laboratory testing. This may embody ankle-brachial indices and segmental pressures (discussed later). Segmental pressures in sufferers with aortoiliac occlusive illness incessantly show blunted waveforms throughout the decrease extremities signifying more proximal illness. Preoperative Planning Angiography is the gold normal for preoperative planning because it can show the precise sample of disease and will assess the patency of the internal iliac arteries. In instances of full aortic or bilateral iliac artery occlusion, brachial entry may be necessary to evaluate the aorta proximal to the occlusion. The widespread femoral artery is most frequently used as inflow, however any artery with in-line circulate from the aorta may be used. More distal vessels should be thought of to lower the size of the bypass, an element associated with elevated vein bypass thrombosis. Runoff may be defined as continuity of the outflow vessel with the foot or, for the peroneal artery, a direct communication between the delta branches and a pedal vessel. Autogenous conduits include the larger and lesser saphenous veins in addition to the basilic and cephalic veins of the arm.
Buy discount prothiaden 75 mg on-line
The projection overlap for the bifurcation is defined by the number of pixels that appear in each the projection of the bifurcation and the projection of the whole coronary tree treatment 001 prothiaden 75 mg with amex. To distinguish between the examples a and c medicine dictionary pill identification cheap prothiaden 75mg, which have related overlap and foreshortening values medicine video quality prothiaden 75mg, a second overlap measure is defined, which is denoted by the internal overlap. This internal overlap determines the overlap that particular person branches of the bifurcation have with each other. The internal overlap for the whole bifurcation is outlined by the utmost value of those pair-wise overlap values. Simulating Angiographic Views the proportion of foreshortening, overlap, and inside overlap for a bifurcation are calculated for a spread of rotation and angulation angles. Left coronary tree with a specific bifurcation area projected from three different angles. Accurate and reproducible measurements are of extreme importance for routine scientific application. A description of select developed methods and the outcomes of various validation studies are introduced subsequently. User Interaction Before performing the automated 3D pathline detection, step one within the evaluation process is to choose the vessel section of curiosity. To simplify the choice, the user needs to define a proximal (start) and a distal (end) point inside the vessel of curiosity in the 3D information space. However, nearly all of this research centered on enhancing the 3D visualization of the vascular constructions in the image, and never on accurate quantification of those buildings. After the proximal and the distal points are outlined, a 3D pathline is routinely detected via the vessel section. The wave propagation speed is ready to be higher in regions of excessive signal depth. Proximal level (in red) and distal point (in blue) represent the user-defined start and finish point of the vessel section of the proper carotid artery. Colorized voxels in the vessel point out the arrival times obtained by applying the wavefront propagation algorithm. The propagation begins on the indicated proximal point and continues until the wavefront reaches the distal level. Using a steepest-descent approach, the optimal trajectory from the distal to the proximal point can be calculated. Therefore, a postprocessing step based on a distance rework is performed to relocate the pathline toward the middle of the lumen. The stomach section was acquired using sequence 1, whereas both peripheral sections had been acquired using sequence 2. Two unbiased observers analyzed the research by specifying the proximal and distal points of the vessel segments. Only the major vessels have been studied, which were the aorta and the widespread iliac, exterior iliac, femoral, and popliteal arteries. In the belly research, three vessels (the aorta and the left and the right widespread iliac arteries) needed to be analyzed. The whole quantity vessel phase to analyze was forty nine segments, 6 of which had to be rejected because no vessel was seen owing to an occlusion of the vessel. After the evaluation was completed, the observers visually inspected the detected centerline and categorized the result as correct or incorrect. It shows that in all however three cases, a correct centerline was detected by each observers. The three failures have been attributable to brighter vessels operating shut and parallel to the vessel of interest and had been identical for each observers. Placing an extra support point in the vessel segment of curiosity was enough to acquire a correct pathline in these instances. Alternatively, the lumen boundaries for small vessel may be detected based mostly on the statement that the intensity on the vessel boundary is roughly 30% of the maximum intensity within the vessel crosssection. In every of these 2D pictures the luminal contour is detected by applying the right threshold. Subsequently, the collection of contours within the 2D cross-sectional pictures is transformed again to 3D house leading to a triangulated mesh, which can be utilized to derive varied quantitative parameters describing the lumen dimensions of the analyzed vessel segment. Based on the utmost intensity within the vessel lumen, near the lumen heart, the vessel boundary is outlined on the location the place the depth is equal to 30% of the utmost value. A downside of the threshold-based approach utilized within the sequence of cross-sectional 2D photographs is that it might result in an unrealistic, irregular, 3D segmentation. In the presence of other vessel operating close to the vessel phase of curiosity or stenotic areas where the utmost intensity at the location of the pathline is low, overestimation of the lumen contour could happen in particular person slices. The tubular mannequin fitting to the cross-sectional photographs is based on a threshold strategy or picture gradient features. By constraining the allowed deformation of the tubular mannequin, such an method is way less delicate to picture artifacts at explicit areas. Promising outcomes of the 3D tubular mannequin fitting has been presented by Makowski and associates. For each of the phantoms, the obstruction diameter was precisely assessed using the automated method with an error of 1. For the regions with an obstruction, nevertheless, overestimation of the diameter occurred for the extra severe stenoses. Given the precise spatial resolution in the order of two � 2 � 2 mm3, the diameter values within the stenotic area of the phantoms with probably the most extreme stenosis correspond to either 1. The results indicate that for accurate diameter measurements, the spatial decision must be such that no much less than three voxel components along the vessel diameter are present. In addition, three different observers independently evaluated the data units utilizing typical measurements of stenosis severity. For computerized evaluation, a stenosis was considered important if the discount in luminal space exceeded 50% of a selected reference segment. This signifies that the automated evaluation performs similarly to conventional evaluation. A, the pink and blue dots characterize the user-defined start and end level of the section to be analyzed. The blue line signifies the reference space, which is an approximation of the lumen area as it will be within the nondiseased state. The p.c stenosis is derived by dividing the precise cross-sectional space by the reference space on the corresponding location. As an alternate, the reference space can be derived from a standard segment distal or proximal to the precise lesion. Accurate detection of the outer wall is, normally, tougher as a result of the intensities of surrounding tissue may be decrease, higher, or have an identical depth as the vessel wall. Alternatively, as a outcome of the form of the outer wall boundary can be approximated by an ellipse, dependable edge info at an area degree is much less necessary. Therefore, for the detection of the outer wall, the first step is to fit an ellipse across the obtainable lumen contour on the picture edges. The ensuing ellipse is then slightly deformed domestically primarily based on a subsequent dynamic programming step. In carotid research of 17 patients,23 a wonderful settlement was observed between contour areas obtained by automated contour detection and contour areas derived from handbook tracings (mean distinction for lumen areas: 9. In addition, in the same study, it was noticed that the agreement of wall thickness measurements between automated detection and guide contour tracing was larger than the agreement between two guide observers. B, Longitudinal reformat view exhibiting the detected luminal boundaries in a stretched view. B, Automatically detected luminal (red) and outer contours (green) and wall thickness measurements using the centerline methodology. A, Automatically detected luminal and outer wall contours in nine consecutive slices. Each contrast-weighting can be optimized in such a means that it targets a selected tissue type inflicting a excessive or low signal excitation of this tissue in comparison with surrounding tissues. For visual plaque assessment, a call scheme can be used just like the one offered in Table 84-3, taking into account the signal intensities in the vessel wall as seen in the numerous sequences. Quantitative analysis of such in depth vessel wall examinations requires: (1) registration of the a number of collection to correct for affected person movement that happens between the series; (2) detection of luminal and outer boundaries in the vessel section of interest; (3) detection and classification of related plaque components; and (4) assessment of parameters precisely describing the vascular pathology.
Purchase prothiaden on line
A treatment eczema order 75 mg prothiaden with visa, the left subclavian artery is occluded proximally and reconstitutes distally (arrow) medicine ball abs cheap prothiaden 75mg amex. B medicine keflex purchase 75mg prothiaden visa, It is clear that the vertebral artery (arrowhead) reconstitutes the subclavian artery (arrow) because the delayed picture (C) reveals less move within the vertebral than in the subclavian artery. Reversal of blood flow through the vertebral artery and its effect on cerebral circulation. Imaging prognosis of subclavian steal syndrome secondary to Takeyasu arteritis affecting a left-side subclavian artery. Cerebral circulatory insufficiency in occlusive processes of the subclavian artery ("subclavian steal impact"). Takayasu arteritis presenting as epileptic seizures: a case report and brief review of the literature. Transcranial Doppler ultrasonography of the basilar artery in patients with retrograde vertebral artery move. Radiological reasoning: extracranial causes of unilateral decreased mind perfusion. Diagnosis of subclavian steal syndrome utilizing dynamic time-resolved magnetic resonance angiography: a technical note. Quantitative magnetic resonance angiography in the analysis of the subclavian steal syndrome: report of 5 patients. Surgical treatment of atherosclerotic lesions of subclavian artery: carotid-subclavian bypass versus subclavian-carotid transposition. Thus, familiarization with various elements of imaging analysis is of extreme significance for the decoding physician. Etiology and Pathophysiology Three primary influences predispose a affected person to thrombus formation, which type the so-called Virchow triad: (1) endothelial harm; (2) stasis or turbulence of blood flow; and (3) blood hypercoagulability. Thus, occlusion of major vessels of greater than 60% of the arterial bed suddenly increases pulmonary artery strain, diminishes cardiac output, and causes right-sided coronary heart failure (acute cor pulmonale) and even demise. The annual incidence of pulmonary embolism is estimated to be between more than 300,000 circumstances, resulting in roughly 50,000 to 100,000 deaths within the United States yearly. Diagnosis of pulmonary embolism remains a clinical challenge because of its nonspecific presentation. D-dimer is a fibrin degradation product that will increase with clot lysis, suggesting the presence of thrombosis. Sensitivity and specificity of a speedy whole-blood assay for D-dimer within the diagnosis of pulmonary embolism. Imaging Techniques and Findings Chest Radiography Initially, the chest radiography findings commonly are normal. However, in later phases, the radiograph could present findings that include a Westermark sign (dilation of pulmonary vessels and a pointy cutoff), atelectasis, a small pleural effusion, and an elevated diaphragm. It denotes focal peripheral lucency beyond an occluded vessel accompanied by gentle dilation of central pulmonary vessels. It is a subtle discovering caused by embolic obstruction or hypoxic vasoconstriction of pulmonary artery. Another discovering is enlarged central pulmonary vasculature, which may be simply missed. It may be attributable to vessel distention by thrombus or by an acute rise in pulmonary arterial pressure secondary to distal emboli. Hampton hump20 is classically referred to as a conical peripheral opacity pointing towards the hilum. These are a number of, subpleural decrease lobe infarcts seen as ill-defined opacities with out air bronchography. These significantly include subsegmental atelectasis (Fleischner lines),21 seen as linear opacities in lung bases; these are transient in nature and thought to be brought on by mucus plugging, hypoventilation, or distant airway closure. Focal air house consolidation represents true pulmonary infarction, with ischemic necrosis or pulmonary hemorrhage with out infarction occurring in 10% to 60% of sufferers. In addition, chest radiographs are used for correlation of the interpretation of V/Q scintigraphy results. B, the arrow factors toward a growing infarct in the posterior segment of right higher lobe. Acute thrombus is commonly anechoic with variable echogenicity, making compression ultrasonography an essential tool for evaluation. The diagnosis is established by lack of venous compression caused by intraluminal thrombus. Lack of applicable response to a Valsalva maneuver additionally signifies thrombosis of the central veins exterior the sphere of view. Normal patent vessels present respiratory phasicity, whereas a monophasic waveform suggests venous obstruction. These studies point out that the air flow scan may be eradicated, thus lowering price and radiation dose. This examine used aerosolized technetium 99m (Tc 99m) for the ventilation portion of the V/Q scan instead of the radioisotope xenon 133. Tc 99m is five occasions smaller in diameter and has a 20% efficiency of pulmonary deposition compared to 2% for xenon 133, thus helping improve the results. It was normally carried out in circumstances of discrepancy between the clinical suspicion and results of the V/Q scan, or if there have been coexisting situations. Angiography was also often performed prior to interventions corresponding to mechanical clot fragmentation. Major problems (1% to 3%) related to the procedure include respiratory misery requiring resuscitation, cardiac perforation, contrast reactions, main dysrhythmias, renal failure, and hematomas. Minor complications (5%) are contrast-induced renal dysfunction, respiratory misery, angina, minor contrast reaction, and transient dysrhythmias. An inspiratory breath-hold is fascinating as a end result of it could improve the pulmonary vascular resistance, resulting in better contrast enhancement. Various concentrations of contrast agent and protocols for injection price have been used, every with its personal advantages and drawbacks. High-contrast agent concentration (300 to 360 mg/mL) with a high fee of infusion (3 mL/second or higher) is the most well-liked, handy, and efficient as a result of it maximizes pulmonary artery opacification and permits using preloaded syringes. Typically, 2- to 3-mm collimation imaging is completed with or without narrow overlapping reconstruction. This technique offers wonderful picture high quality, but additionally leads to a larger data storage requirement. Also, proper timing of the distinction bolus is extraordinarily essential to acquire a high-quality image. Generally, a presumptive scan delay of 20 seconds for higher extremity injections works properly to acquire enough enhancement. Multiplanar reformatted images could be helpful to identify small artery abnormalities, which normally comply with an oblique course, and three-dimensional reconstructions with volume rendering help in displaying advanced anatomy. Small subsegmental emboli will not be detected, although the appearance of faster scanners has allowed even these small and sure clinically insignificant emboli to be readily seen with rising frequency. It has a reported high accuracy, with sensitivity reported to vary from 60% to 100% and specificity from 81% to 100 percent. When it was first developed it represented an necessary advance, because it allows over 90% of sufferers to maintain their breaths throughout the research, thus reducing movement artifact from respiration. Eccentric or peripheral intraluminal filling defects type acute angles with the vessel wall. Occasionally, it might be outlined against this agent when imaged along its axis (railroad monitor sign). Saddle embolus bridges can form across the proper and left primary pulmonary arteries and are a reason for sudden death. This is essential, as a end result of neither V/Q scan nor pulmonary angiography can detect different circumstances reliably. The accuracy of analysis depends on the scale of the artery affected and the dimensions of the emboli (clot burden). It has also been proven to have higher sensitivity and specificity compared to V/Q scintigraphy. A assured analysis can be made in 90% of patients as a result of, even in these in whom a scan is interpreted as negative, an alternative analysis may be established. Controversies concerning the accuracy for diagnosis have been reflected in varied research in several populations (see further discussion in the subsequent section). In this technique, 1 point is given for a clot in every proximal artery, which is equal to every phase arising distally, thus leading to a most rating of 9 for right lung, 7 for left lung, and 16 total.
Cheap 75 mg prothiaden visa
A meta-analysis of randomized controlled trials showed that antihypertensives treatment of scabies order 75mg prothiaden free shipping, including diuretics and blockers medicine 7253 pill buy prothiaden 75 mg with amex, lowered stroke threat by roughly 40% treatment spinal stenosis order generic prothiaden canada. Lipid-lowering remedy is also important to gradual the speed of progression of atherosclerosis and doubtlessly to stabilize plaques. Simvastatin lowered stroke risk by 23% and 25% in the Scandinavian Simvastatin Survival Study (4S) and Heart Protection Study (a study of high-risk patients with atherosclerosis or diabetes), respectively. The remaining statins are thought to have related advantages by way of a class impact. A meta-analysis of 287 trials with one hundred thirty five,000 highrisk sufferers showed a 22% discount in stroke with an antiplatelet regimen. Aspirin plus extended-release dipyridamole is simply as efficient as aspirin alone for lowering demise and nonfatal stroke, but a transparent profit over aspirin is debatable after research with conflicting findings. Certain classes have been shown to have useful results in addition to their blood pressure�lowering effect. Lipid-lowering remedy is another essential element to retard the development of atherosclerosis. Antiplatelet therapy is the third essential drug class that lowers cardiac and vascular occasions; a meta-analysis of 9716 sufferers in forty two trials showed a 23% odds reduction. Oral anticoagulants have minimal elevated profit and an elevated bleeding danger and are contraindicated without an extra applicable indication. Intensive management of different vital comorbid situations, similar to renal disease and diabetes, can markedly reduce occasions. Physician counseling is efficient, leading to a 50-fold enhance in 1-year cessation rates (increase from 0. The addition of nicotine replacement remedy increases the 1-year success rate to 16% and of bupropion to 30%. A meta-analysis of supervised train rehabilitation showed a greater than 180% improve in walking time with simply 30 minutes thrice weekly. Cilostazol is a phosphodiesterase type three inhibitor that improves treadmill time and high quality of life. A meta-analysis of six trials confirmed an improved pain-free walking distance of 30% to 60%. Pentoxifylline (a methylxanthine derivative), L-arginine, propionyl-L-carnitine, and gingko biloba are less effective and never used as incessantly. Aortic Atherosclerotic Disease Aneurysms are the first manifestation of aortic atherosclerotic illness, mostly within the descending aorta. Close surveillance and surgical intervention when the aneurysms reach the appropriate dimension are the primary therapy choices. However, medical remedy is important to slow the progression and to reduce the chance of rupture. Despite its importance, no specific remedy has been shown to reduce the speed of aneurysm development. The best danger components for rupture include tobacco use and uncontrolled hypertension. Ongoing tobacco use will increase the aneurysm development rate by 20% to 25% and considerably will increase the chance of rupture. Renal Atherosclerotic Disease the medical therapy of renal atherosclerotic disease involves both control of the illness course of itself and therapy of the resultant issues. Aggressive atherosclerotic threat issue management is necessary to try to sluggish the development of renal atherosclerosis as for other arterial beds. Resistant, severe hypertension and progressive renal function decline are the 2 main problems of renal atherosclerotic illness and stem from renal artery stenosis. Angiotensin-converting enzyme inhibitors, angiotension receptor blockers, calcium channel blockers, and blockers have all been proven to have some impact on renal artery stenosis�associated hypertension. Both angiotensin-converting enzyme inhibitors and angiotension receptor blockers have been shown to slow the decline in renal function. Medical therapy is often supportive, involving gastric decompression, hemodynamic assist, aggressive intravenous antibiotics, and correction of metabolic acidosis. In uncommon circumstances, intravenous heparin and continuous papaverine infusion (a potent vasodilator) can be utilized with close monitoring. In this case, the dangers of bleeding versus the antiplatelet benefits of aspirin ought to be fastidiously considered. Long-term aspirin use can reduce the danger of recurrent ischemia in the setting of acute or chronic ischemia. Unlike with coronary obstruction, revascularization is indicated solely in sufferers with signs that induce vital way of life or vocational incapacity and have an affordable probability of enchancment with restoration of blood move. Moreover, intermediate lesions should be evaluated with translesional strain gradients with and without vasodilation. There are restricted randomized trial knowledge comparing revascularization to medical therapy. The location of obstructive atherosclerotic disease and lesion characteristics dictate the type of revascularization. The type of revascularization determines the operative mortality and patency rates (Table 88-5). Given surgical dangers and improving technique and technology, there was a shift towards percutaneous approaches. It is currently the first possibility for revascularization but stays imperfect, with a 3% to 7. Individuals with symptoms and carotid stenoses of 70% to 99% had been found to have a 2. Small research with short-term follow-up Transluminal Angioplasty Revascularization Procedure Success and Mortality Rates Operative Mortality Rate (%) three. Transcatheter interventions for the therapy of peripheral atherosclerotic lesions: part I. In the iliac system, surgical procedure is the popular treatment of lengthy or irregular stenoses or occlusions. Comorbid situations such as diabetes, renal failure, and ongoing tobacco use decrease the profit of percutaneous approaches and might influence decision-making. On the other hand, surgery should usually be averted in these younger than 50 years who present with aggressive atherosclerotic occlusive disease; surgical procedure has limited sturdy response on this inhabitants. Aortic Atherosclerotic Disease Medical remedy is essential to help sluggish the development of aortic atherosclerotic disease. However, surgical repair remains the mainstay of therapy for the main complications of aortic atherosclerotic disease: aortic aneurysms and dissections. Although changes for age, gender, and physique floor area are essential, an anteroposterior diameter of 3. Aortic aneurysms can result in thromboembolic ischemic events and impinge on neighboring buildings, however the primary concern is the risk for rupture. Given this dramatic improve in mortality, all symptomatic patients ought to bear restore immediately, no matter aneurysm diameter. For asymptomatic sufferers, surgical decision-making is based on the risk/ profit ratio of procedural morbidity versus chance of rupture, which is immediately related to the maximal diameter, rate of enlargement, and gender of the patient. The threat of rupture for aneurysms smaller than 4 cm is quite low, and surgery may be prevented as these patients usually die of the problems of comorbid cardiopulmonary disease. However, an analysis of 10 main studies reveals an eventual rupture danger for bigger aneurysms that will increase from 20% for aneurysm diameter of more than 5 cm to 50% for these of greater than 7 cm. Monitoring with serial ultrasound research or computed tomography is really helpful every 2 to three years for aneurysms smaller than four cm and each 6 to 12 months for those 4. Two major trials present no profit to surgery for aneurysms with a diameter of lower than 5. Growth rates above 7 to eight mm yearly or a diameter two times the dimensions of the most important normal phase ought to prompt consideration of restore. Given the upper rate of rupture in ladies (up to 4 occasions greater), the American Association for Vascular Surgery recommends consideration of elective restore for aneurysms with diameters as small as four. The morbidity and mortality with this process are presently equivalent to those of open repair. There is an acceptably low danger of rupture however no price financial savings as a result of the need for reintervention stays excessive. However, endografting may be beneficial for those with extreme threat of issues throughout open surgical repair. Thus, open restore is presently really helpful until a high danger for problems is present. Repair of thoracic aortic aneurysms has a higher danger of morbidity and mortality, which makes medical and percutaneous remedy preferential.
Cheap 75mg prothiaden otc
Comparison of Rb-86 and microsphere estimates of left ventricular blood move distribution medications erectile dysfunction purchase 75 mg prothiaden free shipping. Noninvasive evaluation of coronary stenoses by myocardial imaging during pharmacologic coronary vasodilation medicine 801 buy prothiaden 75mg on line. Detection of coronary artery illness in human beings with intravenous N-13 ammonia and positron computed tomography medications 126 cheap prothiaden 75 mg on-line. Detection of coronary artery illness with 13N-ammonia and high-resolution positron-emission computed tomography. Positron emission tomography for the diagnosis of coronary artery disease: a non-university experience and correlation with coronary angiography. Noninvasive estimation of regional myocardial oxygen consumption by positron emission tomography with carbon-11 acetate in patients with myocardial infarction. Assessment of myocardial fatty acid metabolism with positron emission tomography at rest and during dobutamine infusion in patients with coronary artery disease. Altered myocardial fatty acid and glucose metabolism in idiopathic dilated cardiomyopathy. Reduced myocardial carbon-11 hydroxyephedrine retention is associated with poor prognosis in chronic heart failure. Radiation dose to technicians per nuclear medicine procedure: comparability between technetium99m, gallium-67, and iodine-131 radiotracers and fluorine-18 fluorodeoxyglucose. Pharmacologic Stress Agents Alexander Bustamante and Gautam Nayak* As imaging modalities for the detection of coronary heart illness continue to evolve and the elderly patient population expands, alternatives to traditional train stress testing have gotten extra essential in clinical practice. Increasingly, patients with situations precluding train treadmill testing are being referred for diagnostic evaluations for attainable coronary artery disease using pharmacologic stress tests. Exercise stress imaging provides important diagnostic and prognostic data and is right for otherwise in a position sufferers. Not all patients can tolerate the rigorous exercise inherent in an exercise treadmill take a look at, nevertheless. In these sufferers, including sufferers with degenerative joint disease, pulmonary conditions, peripheral vascular disease, congestive heart failure, and different systemic processes that stop the attainment of adequate train stress ranges, pharmacologic brokers have turn into pivotal. Two major categories of pharmacologic brokers are most incessantly used: vasodilators and inotropes. Although each forms of agents can be used in either stress perfusion imaging or stress echocardiography, vasodilators have found their area of interest in nuclear perfusion research, and inotropes have turn out to be more common in stress echocardiography. This chapter explores each kinds of pharmacologic stress brokers from their physiologic foundation to their diagnostic and prognostic value. The medical implications of each modality and their inherent advantages and disadvantages are particularly emphasized. The two brokers most extensively studied and in present scientific use are adenosine and dipyridamole. Their utility continues to grow primarily based on a wealth of scientific proof and expanding indications and imaging modalities. This pulsatile move is performed by way of a highly curved, branching vascular system composed of larger epicardial vessels and smaller intramural vessels. While epicardial coronary arteries function conductance vessels, intramural arteries distribute and regulate blood move. This adaptation, termed autoregulation, happens rapidly in response to modifications in myocardial oxygen calls for, primarily through functional hyperemia. Coronary Flow Reserve As atherosclerosis develops in epicardial coronary arteries, the ensuing stenosis produces resistance to blood circulate. The flow improve in response to vasodilators in vessels with a mild-to-moderate stenosis may still be two to three times regular due to coronary move reserve. This prevents differentiation with a traditional coronary artery owing to radiotracer roll-off at a fixed level of hyperemic flow as a result of the conventional and mildly stenotic arteries would have identical tracer uptake. Theophylline and caffeine act at these receptors as aggressive blockers, decreasing the effects of adenosine. Clinically, adenosine is infused intravenously and has a very short half-life of lower than 2 seconds. Adenosine is given typically as a continuous infusion of 140 �g/kg/min for 4 to 6 minutes, with radiotracer injection midway into the infusion. To keep away from an unintended speedy bolus of residual adenosine, radionuclide dose injection and flushing and adenosine infusion ought to be accomplished by way of separate intravenous traces or by way of using a twin port. Side effects are frequent with adenosine infusion, occurring in more than 75% of patients (Table 26-1). These unwanted side effects are transient, often resolving inside 1 to 2 minutes of stopping the infusion, and barely require reversal with aminophylline. Most unwanted aspect effects are related to stimulation of the adenosine A1 and A3 receptors. Although stimulation of the adenosine A3 receptors can theoretically lead to bronchospasm, most dyspnea occurring with adenosine infusion is in all probability going related to hyperventilation. Most bradyarrhythmias are transient and resolve despite continued adenosine infusion. Physiologic foundation for assessing crucial coronary stenosis: instantaneous circulate response and regional distribution throughout coronary hyperemia as measures of coronary move reserve. This concept of coronary circulate reserve is integral to understanding the physiologic effects of chronic atherosclerosis within the lumen of the coronary tree. The response of coronary arteries to vasodilators is decided by the diploma of stenosis and the chronic effects of coronary circulate reserve at the time of vasodilator administration. The practical impact of this "roll-off" in the uptake-flow relationship is a Dipyridamole Dipyridamole is a pyrimidine base that induces vasodilation by elevating blood and interstitial levels of adenosine. B, Myocardial flow with hyperemia will increase four occasions above resting flow in the arteries with no coronary artery illness. In the territory supplied by the stenotic artery, hyperemic move will increase only twofold. As a end result, radiotracer uptake is relatively decreased within the territory supplied by the stenotic vessel, leading to a perfusion defect. The adenosine A2a receptor mediates coronary arteriolar vasodilation, which is the idea for pharmacologic stress testing. Alternatives to leg exercise in the analysis of sufferers with coronary artery disease: practical and pharmacological stress modalities. Activation of the adenosine A2 receptor leads to a fancy sequence of events mediated by G proteins and leading to a lower in intracellular calcium uptake, culminating in coronary vasodilation. This is distinct from adenosine, where tracer injection is throughout vasodilator infusion. The standard intravenous dose of dipyridamole leads to a slight enhance in coronary heart fee, a decrease in systolic blood stress, a modest enhance in cardiac output, and a slight enhance in pulmonary capillary wedge pressure. Side effects occur in about 50% of sufferers and embrace chest pain, nausea, dizziness, and headache (see Table 26-1). Dipyridamole has usually been extensively studied and has a wonderful safety document. Most vital unwanted effects could be reversed with sluggish intravenous administration of theophylline (100 to 300 mg), which is a aggressive blocker of adenosine receptors. Norepinephrine stimulates 1 receptors located on the cardiac cell membrane resulting in a complex protein signaling cascade that ends in the enhancement of calcium entry into the cell. Calcium potentiates the motion between actin and myosin growing myofibril contraction. Echocardiographic images are typically obtained firstly of the dobutamine infusion, and at prespecified intervals to embrace peak heart price and restoration phases. The 1-adrenergic receptor is illustrated with direct coupling through Gs to voltage-sensitive Ca2+ channels. The actions of particular inotropes depend on the balance of and exercise, which predominantly mediates peripheral vasoconstriction. Other catecholamines stimulate 2 receptors situated in vascular clean muscle and result in vasodilation. Hypotension can happen in some sufferers, but due to the brief halflife of dobutamine, this typically resolves on discontinuation of the infusion. As a end result, this agent has been used extensively in patients with decompensated coronary heart failure without profound hypotension. The extra 2 properties might end in aggravating preexisting hypotension, and may require the need for concomitant 1 stimulating vasoconstrictors to improve peripheral arterial resistance. At larger doses of dobutamine, coronary heart rate is incrementally elevated through 1 stimulation. The mixture of inotropic and chronotropic results ends in an increase in myocardial oxygen demand with secondary coronary vasodilation making for an efficient stress agent.