Co-Director, UT Health San Antonio Joe R. and Teresa Lozano Long School of Medicine
In addition, distinction pericardiography, as quickly as the epicardial entry is obtained, can help delineate the anatomy and assess for the presence of adhesions, which can limit catheter navigation. Ventral aspect of the pericardium with the anterior portion of the pericardial sac and the heart eliminated to show the good vessels on the base of the guts. The ventral floor of the transverse sinus is formed by the posterior aspect of the ascending aorta and the inferior�posterior floor of the right and left pulmonary arteries before they emerge from the pericardial sac. Mapping of the atrial floor can be limited by the normal pericardial reflections and by the atrial irregular atrial anatomy (right and left atrial appendages). Careful catheter manipulation and sheath management are crucial to assist avoid aspiration of air into the epicardial space and to avoid laceration of the epicardial vessels. When using stiff sheaths in the epicardial area, it is suggested to lead with a wire or ablation catheter before advancing or shifting the curl of the sheath. Also, it is recommended to not go away a large sheath within the pericardial space and not using a catheter in place because the sides of the sheath can doubtlessly lacerate epicardial vessels or the myocar dium itself. In these circumstances, a hybrid procedure involving surgical entry with a subxiphoid pericardial window or a restricted anterior or lateral thoracotomy, and handbook dissection and lysis of the adhe sions can facilitate entry to the epicardial area of interest. However, the presence of pericardial adhesions between the parietal and visceral serosal surfaces. Whereas the pericardial adhesions in postpericarditis sufferers are often diffusely distributed, adhesions in postsurgical patients are largely concentrated within the anterior portion of the guts (the area where the pericardial sac was opened during sternotomy). Importantly, even when epicardial entry is possible, the presence of pericardial adhesions can considerably limit catheter maneuverability inside the pericardial house. This method may help increase the epicardial areas accessible for mapping and ablation. Flow of intraperi cardial contrast dye on repeat injection helps assess efficient disruption of the adhesions. Care should be taken to avoid cardiac perforation with the catheter tip in these instances. Furthermore, in patients with prior coro nary bypass surgical procedure, dense adhesions sometimes occupy the area of the coronary graft, hindering epicardial access to that region. In these patients, you will want to perform coronary native vessel and graft angiography to outline anatomy and keep away from graft disruption by catheter manipulation. It is also essential to note that, in patients with coronary artery occlu Epicardial Fat Epicardial fats is the adipose tissue positioned between the visceral pericar dium and the myocardium. Epicardial fats covers 80% of the center floor, with a imply thickness of the fat layer of 5. There is a broad individual variation within the quantity and distribution of epicardial fats. First, interposed between the mapping catheter and myocardium, epicardial fat dampens recorded electrogram amplitude as well as the ventricular stimulation threshold, hindering activation and tempo mapping methods and making it dif ficult to differentiate fats from true scar. Pericardial entry is carried out (anterior approach) in a patient with biventricular pacemaker and prior episode of pericarditis. Note that the contrast dye injected initially through the pericardial access needle remained stagnant at the anterior side of the heart, and the guidewire coiled in the identical area, as a end result of compartmentalization of the pericardial area secondary to pericardial adhesions. The following discussion highlights certain peculiarities pertaining to the percutaneous epicardial approach to mapping. Epicardial mapping of native activation timing and electrogram morphology employs prin ciples much like those of endocardial mapping. However, because of the presence of epicardial fats, low electrogram amplitude might not have the identical implications as these during endocardial mapping (see below). Entrainment and Pace Mapping Entrainment and tempo mapping maneuvers are normally troublesome to carry out using bipolar pacing because of a very excessive epicardial stimulation threshold (>15 mA) in the majority (approximately 70%) of instances, and are doubtless associated to the presence of epicardial fats and poor catheter contact because of freedom of catheter movement within the pericardial space. With unipolar pacing, the pacing threshold generally is less than 10 mA at 2 milliseconds in regular tissue. A consultant instance of endocardial (A) and epicardial (B) electroanatomic activation maps is shown from a affected person nonischemic cardiomyopathy. A considerably wider endocardial space of early activation is observed in comparison with epicardial activation. The voltage map reveals surface reconstruction of the anterior surface of the heart. There is a low-voltage space (red) extending from the best ventricular outflow tract to the apex and following the lateral inferior margin to the bottom of the best ventricle. Areas of infarction or scar have lowamplitude elec trograms just like findings throughout endocardial mapping. However, epicardial fats, which is concentrated along the coronary sulcus and the interventricular grooves, can cause lowamplitude electrograms, falsely suggesting scar in voltage maps. Normal epicardial electrograms dem onstrate bipolar signal amplitude usually above zero. However, in areas with a layer of epicardial fats greater than 5 mm in thickness, the amplitude of the recorded bipolar epicardial electrogram can lower, which can confound the power to discriminate between fats and scar. Therefore to keep away from a misclassification of lowvoltage areas as a end result of epicardial fat or major coronary vasculature as irregular, it is necessary to analyze the location and extent of the confluent voltage abnormality as properly as the electrogram morphology characteristics. The presence of abnormal electrograms (fractionated, cut up, or late potentials) is normally a more reliable indicator of scarring. While endo cardial bipolar mapping is capable of assessing local electrograms originating from tissue adjoining to the recording electrodes. Nonetheless, the presence of epicardial fat interposed between the catheter tip and the myocardial tissue solely reasonably attenuates the efficacy of cooled tip ablation. Commonly, the flow fee is ready at 0 to 1 mL/min throughout mapping and at 10 to 17 mL/min throughout ablation, and is titrated as required to preserve the electrode temperature at less than 50�C. Monitoring for an impedance fall is commonly used to assess adequacy of energy supply. This may be achieved by intermittently eradicating the ablation catheter to permit aspiration from the pericardial sheath or placing a second pericardial catheter for drainage functions. Evaluation of the pericardial space can be performed by intra cardiac or transthoracic echocardiography, and by injecting 2 to three mL of contrast under fluoroscopy, to affirm full drainage earlier than removing the sheath. Generally, no main reaccumulation of pericardial fluid is noticed following submit procedure draining of the pericardial fluid. After controlling the bleeding, moni toring the affected person with serial transthoracic echocardiography over the following 24 hours is beneficial. Antibiotic remedy is administered postprocedure and so long as a drain is left in the pericardial area. Complications of Transthoracic Epicardial Ablation Acute complications associated to the epicardial strategy have been reported in about 9% of instances at experienced centers, and may be associated to the pericardial entry process or to catheter manipulation or ablation inside the pericardial house. Furthermore, careful catheter manipulation main with a wire or ablation catheter earlier than maneuvering the curl of the pericardial sheath can help scale back the chance of damage to the myocardium and epicardial vessels. The amount of blood drained from the pericardial area usually ranges from 20 to 300 mL. Therefore precau tions must be in place for managing extreme bleeding, including the supply of acceptable surgical expertise. The drain could additionally be removed as soon as the absence of reaccumulating effusion is verified on echocardiographic examinations over a 24hour interval. Therefore leaving a pericardial drain in place for several hours also could additionally be con sidered even in sufferers with no proof of pericardial effusion or intrapericardial bleeding at the end of the procedure. However, such a apply should be balanced in opposition to the chance of pericarditis, infection, and patient discomfort associated with a persistent drain. However, human expertise is proscribed, and extra research are needed to assess security and efficacy. The anterior and posterior septal and basal ventricular areas, the place coronary arteries and veins are identified to traverse, are the extra dangerous zones. Extrinsic compression of a coronary artery can even outcome from edema caused by close by ablation. Based on available data and experience, a distance of at least 5 mm between the coronary artery and the ablating electrode (at any point of the cardiac cycle throughout coronary angiography and in a minimum of two projections) is usually accepted. However, these medication are usually used during the induction of anes thesia, and their results have dissipated by the time ablation is being performed. Mechanical separation of the phrenic nerve from adjoining buildings, using a large balloon, involves insertion of a wire though one of many current peri cardial sheaths to the neighborhood of the ablation catheter positioned at the target epicardial website. Another methodology is to introduce a mixture of saline and air into the pericardium to obtain a "controlled" hydro pneumopericardium to increase the distance between the phrenic nerve and the ablation target area.
Studies using verapamil, digoxin, or procainamide confirmed no important benefits in comparability with a placebo. When antiarrhythmic drug remedy is required for rhythm management, amiodarone is the drug of selection. Generally, oral beta-blocker remedy is began at least 2 to 3 days before surgical procedure, or within 24 hours after surgery if not given preoperatively. In sufferers already receiving continual beta-blocker therapy, the drug must be continued without interruption perioperatively. Oral regimens have been began at 1, 5, or 7 days earlier than nonemergent surgery and continued for a quantity of days postoperatively. Sotalol remedy is normally began 24 to forty eight hours before surgery or four hours after surgical procedure. Most of these sufferers have a quantity of stroke danger elements but additionally elevated threat of bleeding in the postoperative phase. Ambulatory cardiac monitoring ought to be considered to display screen for asymptomatic paroxysmal arrhythmias. Atrial fibrillatory activity is generally best seen in lead V1 and in the inferior leads. With up to 600 impulses generated every minute, syncytial contraction of the atria is replaced by irregular atrial twitches. Therefore the fibrillating atria appear to be a bag of worms in that the contractions are very speedy and irregular. The f waves vary in amplitude, morphology, and intervals, thus reflecting the multiple potential forms of atrial activation which may be present on the identical time at different locations all through the atria. The ventricular price in untreated sufferers normally ranges from 90 as a lot as one hundred seventy beats/min. Ventricular rates which might be clearly outdoors this vary recommend some concurrent influence. Other investigators confirmed that the ventricular response also is dependent upon atrial enter frequency. Rarely, the R-R interval can be regularly irregular and present group beating with the mix of full heart block and a decrease nodal pacemaker with a Wenckebach kind of exit block. Infrequently, impulses from the decrease pacemaker journey alternately down the proper and left bundle branches or alternate fascicles of the left bundle department, resulting in a bidirectional tachycardia. This arrhythmia, which can be incessantly a reflection of marked digitalis toxicity, may seem to be ventricular bigeminy. In true bigeminy, however, the ventricular beat in the bigeminal sample is premature. In comparability, the R-R interval is common with a bidirectional tachycardia as a end result of all the beats come up from a single pacemaker. Aberrancy is brought on by the physiological changes of the conduction system refractory durations that are associated with sudden changes in heart fee. Thus there can be aberrant conduction from a protracted R-R interval adopted by a brief cycle. In this scenario, the refractory period of the bundles will increase through the long R-R interval (long cycle). The presence or absence of a long-short cycle sequence is probably not helpful in differentiating aberration from ectopy for two causes. The proper analysis of aberrant conduction is a continuing challenge, however it could usually be achieved by cautious evaluation of the rhythm strip and utility of certain criteria. Targeting these triggers by either focal ablation or electrical isolation of the involved thoracic veins has been tried in chosen patients. With the success of the Cox-maze procedure, a number of variations of the procedure have been carried out, most of which have involved using a smaller lesion set. The success of surgical linear lesions led to the event of the catheter-based approach to carry out linear ablation. Although the efficacy was modest, complication charges were excessive, and process and fluoroscopy instances have been exceedingly long, this report demonstrated a proof of idea that led others to try to enhance the catheter-based strategy. In the late Nineteen Nineties, Pappone and coworkers developed the wide-area circumferential ablation strategy utilizing three-dimensional (3-D) electroanatomic mapping. However, reaching that is technically difficult and requires lengthy, arduous procedures. However, a longer interval (approximately 6 months) is required for amiodarone, which will not be sensible. Continuing antiarrhythmic drug remedy after ablation can potentially cut back the incidence of early recurrences of symptomatic atrial arrhythmias and the need for cardioversion or hospitalization for arrhythmia administration. On the other hand, anticoagulation can enhance the chance of hemorrhagic complications, together with hemopericardium, pericardial tamponade, and vascular problems. Therefore rigorous periprocedural anticoagulation is of paramount significance to stop thromboembolic occasions whereas minimizing hemorrhagic problems. Alternatively, protamine may be administered to reverse heparin effects (1 mg of protamine for each a hundred models of heparin received within the previous 2 hours). Hemostasis could be achieved by either direct strain or the usage of a figure-of-8 suture. Although some reviews confirmed that discontinuation of anticoagulation remedy 3 months after profitable catheter ablation may be secure over mediumterm follow-up in some subsets of patients, this has not been confirmed by a large prospective randomized trial and therefore remains unproven. Uninterrupted anticoagulation strategies eliminate a interval of inadequate anticoagulation immediately following the ablation procedure, and it doubtlessly reduces the risk of acute bleeding problems by obviating the need for heparin or enoxaparin remedy after ablation. In addition, recent proof suggests that unfractionated heparin shows unexpected slow anticoagulation kinetics in a big proportion of sufferers for up to 20 minutes after infusion. Hence, many operators now favor complete heparinization after vascular access, and clearly before transseptal puncture. Therefore long-term cardiac ambulatory monitors to display for asymptomatic occurrences of atrial arrhythmias must be considered. Postprocedural Electrocardiogram Monitoring Patients are typically hospitalized the night after the process, with cardiac monitoring, and discharged home the next day. After hospital discharge, the strategy and frequency of cardiac monitoring is determined by particular person needs and the results of arrhythmia detection. On the other hand, arrhythmia monitoring to assess the efficacy of the ablation process is typically delayed for at least three months following ablation as a result of early recurrences of atrial arrhythmias are frequent in the course of the first 1 to three months after ablation and a lot of of them resolve spontaneously. Technical Aspects Common to Different Methods of Ablation Sedation During Ablation In most sufferers, deep sedation or general anesthesia is used to prevent patient actions during long and doubtlessly painful procedures and enhance catheter and mapping system stability. Furthermore, phrenic nerve stimulation, if performed, can cause significant movement in nonanesthetized sufferers. The latter technique can potentially improve the risk for embolic occasions as a end result of manipulation of the sheath introducing air or thrombi. Ultimately, nevertheless, the choice of imaging modality is dictated by local availability. It is regularly necessary to apply clockwise torque to each the catheter and its long sheath. Care have to be taken to not permit the round (Lasso) catheter to cross the mitral annulus as a end result of it could possibly then become trapped with the mitral valve apparatus. Usually, reversal of the catheter movement (clockwise torque) that resulted on this situation helps right it. A more limited ablation strategy requires shorter procedure and fluoroscopy instances and could be safer. Cryoablation has additionally been used to target these websites although the precision of mapping is much less (6-mm catheter tip). V3 V4 V5 Endpoints of Ablation the endpoint of ablation is elimination of ectopy, spontaneous or induced by provocative maneuvers (using both the identical provocative maneuvers and defibrillation protocols as earlier than the ablation). In addition, there could additionally be a paucity of spontaneous or inducible arrhythmias through the procedure. Remapping often shows new foci within the ablated vein or in other veins, rather than recurrence of the original focus. The spike is typically localized, and its amplitude quickly decreases when the catheter tip is turned or moved a number of millimeters. Bystander or far-field activity from contiguous branches may be distinguished by temporal delay or lower amplitude. A second electrogram component with a gradual deflection (depolarization rate [dV/dt] of less than 0. Mechanically induced beats could be prevented by avoiding manipulation of the catheters in the course of the recordings.
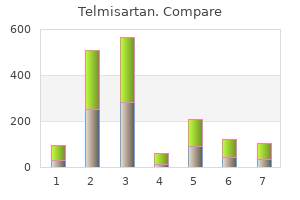
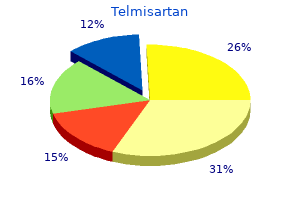
Telmisartan 80 mg lowest price. Blood Pressure Medication Recalled After Trace Amounts of Cancer-Causing Chemical Found.
Predialysis blood stress and mortality risk in a national sample of upkeep hemodialysis patients. Changing relationship of blood pressure with mortality over time amongst hemodialysis sufferers. Systolic blood stress and mortality in chronic hemodialysis patients: results of a nationwide italian research. Effect of pravastatin on cardiovascular occasions in individuals with continual kidney illness. Pravastatin for secondary prevention of cardiovascular occasions in persons with delicate chronic renal insufficiency. Salutary effects of hemodialysis on low-density lipoprotein proinflammatory and high-density lipoprotein anti-inflammatory properties in affected person with end-stage renal illness. Dyslipidemia of continual renal failure: the nature, mechanisms, and potential consequences. Lipoprotein(a) concentrations, apolipoprotein(a) isoforms and scientific endpoints in haemodialysis patients with kind 2 diabetes mellitus: results from the 4D Study. Reverse epidemiology of cardiovascular danger elements in upkeep dialysis patients. Association between cholesterol level and mortality in dialysis sufferers: function of irritation and malnutrition. Hypocholesterolemia is a significant predictor of dying in a cohort of persistent hemodialysis patients. Kidney disease: enhancing world outcomes lipid guideline development work group M. Secular developments in cardiovascular mortality charges of patients receiving dialysis in contrast with the general population. Congestive coronary heart failure in dialysis sufferers: prevalence, incidence, prognosis and danger factors. Comparative survival of dialysis sufferers within the United States after coronary angioplasty, coronary artery stenting, and coronary artery bypass surgery and impression of diabetes. Comparison of short- and long-term outcomes of coronary angioplasty in patients with and with out diabetes mellitus and with and without hemodialysis. Glycemic management and extended hemodialysis survival in sufferers with diabetes mellitus: comparative outcomes of traditional and time-dependent Cox mannequin analyses. Clinical apply guidelines and medical apply suggestions for diabetes and persistent kidney illness. Diabetic kidney disease: a clinical update from kidney illness: improving global outcomes. Cardiac troponin T and C-reactive protein for predicting prognosis, coronary atherosclerosis, and cardiomyopathy in sufferers undergoing long-term hemodialysis. Changes in left ventricular mass in youngsters and adolescents throughout persistent dialysis. Prognostic impression of the indexation of left ventricular mass in patients undergoing dialysis. Regression of left ventricular hypertrophy after conversion to nurnal hemodialysis. Reduction of left ventricular diameter and mass after surgical arteriovenous fistula closure in renal transplant recipients. Effect of hemoglobin ranges in hemodialysis sufferers with asymptomatic cardiomyopathy. Smoking: a risk issue for progression of chronic kidney illness and for cardiovascular morbidity and mortality in renal patients-absence of evidence or evidence of absence Smoking and cardiovascular outcomes in dialysis patients: the United States Renal Data System Wave 2 Study. Oxidative stress in end-stage renal illness: an rising menace to patient outcome. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal illness. Cardiac output and associated left ventricular hypertrophy in pediatric chronic kidney disease. Serial cardiac affect of quantity overload induced by interventional remedy for central venous stenosis or occlusion in chronic hemodialysis sufferers. Long-term cardiovascular changes following creation of arteriovenous fistula in sufferers with end stage renal disease. Albuminuria is independently associated with cardiac reworking, abnormal proper and left ventricular perform, and worse outcomes in coronary heart failure with preserved ejection fraction. The reliability and validity of echocardiographic measurement of left ventricular mass index in hemodialysis patients. Threedimensional echocardiographic analysis of left ventricular function throughout hemodialysis. Left ventricular mass and systolic perform in kids with persistent kidney disease-comparing echocardiography with cardiac magnetic resonance imaging. Comparative evaluation of 2-dimensional echocardiography vs cardiac magnetic resonance imaging in measuring left ventricular mass in patients with and without end-stage renal disease. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective research. Inflammation, malnutrition, and cardiac illness as predictors of mortality in hemodialysis patients. Comorbidity and acute medical events as determinants of C-reactive protein variation in hemodialysis sufferers: implications for affected person survival. Wishful thinking: the surprisingly sparse proof for a relationship between oxidative stress and heart problems in hemodialysis patients. Inflammation and cardiovascular occasions in people with and without chronic kidney disease. C-reactive protein and albumin as predictors of all-cause and cardiovascular mortality in chronic kidney disease. Heart Outcomes Prevention Evaluation Study I, Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P. The antioxidant acetylcysteine reduces cardiovascular events in sufferers with end-stage renal failure: a randomized, managed trial. Vitamin E-bonded hemodialyzer improves neutrophil function and oxidative stress in patients with end-stage renal failure. Hemodialysis impairs endothelial function by way of oxidative stress: results of vitamin E-coated dialyzer. Putative function of uneven dimethylarginine in microvascular disease of kidney and heart in hypertensive sufferers. Endothelium-dependent and -independent vascular operate in advanced chronic kidney disease. Asymmetric dimethylarginine and development of chronic kidney illness: the gentle to reasonable kidney illness study. Asymmetrical dimethylarginine predicts progression to dialysis and dying in sufferers with persistent kidney illness: a competing dangers modeling approach. Asymmetric dimethylarginine and mortality in stages 3 to 4 continual kidney illness. Effect of simvastatin on plasma uneven dimethylarginine focus in patients with chronic kidney illness. Nonfasting plasma whole homocysteine ranges and stroke incidence in elderly persons: the Framingham Study. Nonfasting plasma whole homocysteine levels and all-cause and heart problems mortality in elderly Framingham women and men. Effect of homocysteine lowering on mortality and vascular disease in superior chronic kidney illness and end-stage renal illness: a randomized controlled trial. Homocysteine-lowering and cardiovascular disease outcomes in kidney transplant recipients: main outcomes from the folic acid for vascular end result reduction in transplantation trial. Effect of folic acid and B vitamins on threat of cardiovascular occasions and complete mortality amongst ladies at excessive threat for cardiovascular disease: a randomized trial. Phosphate binder choice in dialysis sufferers: a name for evidence-based quite than marketing-based scientific apply.
Management and outcomes of patients present process surgery for traumatic cervical fracture-subluxation associated with an asymptomatic vertebral artery injury. The management of vertebral artery damage in anterior cervical backbone operation: a scientific evaluate of revealed instances. Bono Abstract Intimate awareness amongst gamers, athletic organizations, and health care providers about sports-related cervical backbone accidents is the vital thing for prevention, management, and knowledgeable decision-making about return to play. Treatment selections can have vital well being, psychological, and financial implications for scholastic and skilled athletes alike. Athletes with underlying cervical canal stenosis are at specific risk for spinal twine neurapraxia, characterised by transient motor and/or sensory deficits in all 4 extremities. Physicians and first responders at organized sporting occasions ought to have established protocols for emergent initial assessment and treatment strategies in the event of an on-field injury. Athletes with suspected cervical spine accidents ought to endure neurological analysis and be handled with spinal precautions to forestall secondary harm. Factors influencing return-to-play selections ought to be particular to the athlete, underlying anatomy, damage sort, and sport, while considering the diploma of ongoing symptoms. Although some accidents can be profession ending, many athletes are often capable of return to sport after applicable treatment, supplied the potential for substantial reinjury is minimized. Prudently, an athlete should be healed, reveal a neurologically intact exam, be freed from ache, and have full power and range of movement prior to returning to sport. Keywords: spinal twine harm, sport accidents, cervical fractures, sprains and strains, burners, cervical cord neurapraxia, cervical disc herniations has decreased over time because of increased public awareness, safer guidelines governing play, and improved protective gear. Tackling and blocking are two of probably the most frequent mechanisms that end in cervical accidents in American soccer. Unfortunately, a rise within the price of catastrophic cervical spine accidents coincided with the appearance of recent helmets as head safety inspired playing methods that enabled use of the highest of the helmet because the preliminary point of contact for blocks and tackles. Although cervical spine accidents are commonest in athletes who take part in organized contact and collision sports, such as rugby, American soccer, and hockey, they regularly occur in those additionally who take part in noncontact sports, similar to baseball, gymnastics, biking, skiing, snowboarding, and diving. While organized sports activities accidents are well studied, the injuries that happen during recreational sporting actions are likely underreported however could be just as devastating. The straightened cervical backbone (in sort out position) allows axial load to be immediately transmitted to the anterior cervical vertebrae which obviates a big diploma of posterior soft-tissue energy absorption. The imply time missed for play was one hundred twenty days for a cervical fracture and 85 days for cervical disc degeneration/ herniation. The reported traumatic quadriplegia rate was 5 per one hundred,000 high school athletes and 1 per a hundred,000 faculty athletes. In 2002, the incidence of traumatic quadriplegia for high school athletes and faculty athletes was down to 0. Furthermore, distortions in measurements might occur in patients with cervical muscle spasms; whereas in youthful athletes, additional physiologic ligamentous laxity can result in pseudosubluxation. At that time, if the athlete is free of ache and has full vary of movement with out radiographic instability, sports activities could be resumed. Though considerably exterior the scope of this chapter, detecting occult cervical ligamentous injuries in obtunded injured athletes deserves some mention. An unconscious participant ought to be handled as though the cervical spine is unstable until proven otherwise. Strict spinal precautions are instituted, together with placement on a rigid backboard, whereas the affected person is transferred to a trauma center. Protective helmets and shoulder pads worn by some gamers can hinder initial evaluation. If the injured athlete is wearing a helmet, the facemask should be removed to facilitate access to the airway, nevertheless the helmet itself ought to stay in place till there are a quantity of folks available to assist with its removing in a managed environment, normally in a hospital setting. To guarantee appropriate alignment, the helmet and shoulder pads must be removed on the identical time to avoid undue flexion or extension of the neck. Improper handling of an unstable cervical backbone could result in further displacement and doubtlessly worsening of neurological injury and even result in cardiopulmonary compromise. Stable cervical spinal fractures involving a spinous course of or lamina could be handled symptomatically. In such instances, flexion and extension radiographs should be obtained to rule out ligamentous injury. Sports may be resumed once osseous therapeutic is full and painless vary of movement is restored. The useful limitations and risks of adjoining damage following higher cervical fusion represent one of the absolute contraindications to return-to-play. Axial load mechanisms are a common explanation for sports-related cervical backbone morbidity. The response of the backbone to utilized axial load depends on the position of the neck at the time of injury. Axial forces applied across a relatively flexed neck lead to flexion forces on the anterior elements and distractive forces on the posterior elements. Energy from this mechanism may end in a so-called teardrop fracture involving the anteroinferior vertebral body7 while simultaneously inflicting distractive harm to the posterior constructions. Disruption of the stabilizing posterior soft-tissue elements, together with the supraspinous ligament, interspinous ligaments, and aspect capsules, is the crucial element resulting in instability and choices concerning management. Disruption of the posterior ligamentous buildings with out vertebral physique fractures can result in bilateral facet subluxation 14. Regardless of the exact mechanism, disruption of the posterior ligamentous complicated usually necessitates surgical stabilization to restore stability. Axial load applied throughout a neutrally aligned neck is extra prone to lead to a compression fracture of the vertebral physique. Surgical stabilization may be required to mitigate progressive deformity progression. While not exactly cervical backbone injuries, both describe common athletic injuries from insult to the brachial plexus or an exiting cervical nerve root, resulting in sudden nondermatomal pain and paresthesias in a single extremity. The defining attribute that differentiates burners from a central spinal cord course of is the involvement of only one extremity. In athletes with recurrent or chronic burners, the etiology is extra more doubtless to be the results of nerve root compression in the intervertebral neuroforamina secondary to cervical disc disease. Electromyography may be considered for athletes with more than a quantity of weeks of persistent signs to decide the presence of a cervical root injury versus brachial plexopathy. Athletes might return to sport after resolution of signs provided they show full energy and range of movement. The athlete and training workers must be recommended that recurrence remains unpredictable and is a threat. Modification of tackling methods, in conjunction with rehabilitation and paraspinal muscle strengthening, could also be efficient in preventing or reducing the rate of recurrence. Neurological signs involving more than one extremity should prompt concern for spinal wire involvement. Cervical spinal cord neurapraxia has been estimated to occur in 7 per 10,000 soccer gamers. Hyperextension may cause an inward buckling of the ligamentum flavum leading to twine compression. Athletes can also have congenital situations such as Klippel�Feil syndrome which refers to a failure of cervical vertebral segmentation, resulting in a reduced variety of segments amongst which to dissipate load. Of notice, whatever the presence of transient quadriplegia, both Klippel�Feil syndrome and dens hypoplasia are absolute contraindications to participation involved sports activities. Horizontal C3�C4 cervical side orientation and relative hypermobility of the neck in extension have additionally been implicated as contributing factors for transient quadriparesis. However, no subsequent everlasting neurological deficits had been reported over the following follow-up interval. These athletes, by advantage of the neuropraxic occasion, have successfully demonstrated diminished functional neurological capability for contact sports. Athletes with ligamentous instability and a historical past of cervical twine neurapraxia without appreciable central stenosis, should also refrain from contact sports activities. Consideration for return-to-play is given to athletes with full neurological restoration with out proof of spinal stenosis, cord compression/ edema, or ligamentous laxity. Noncontact sports could have a protecting effect against cervical disc herniations due to elevated dynamic muscular support of the cervical spine.