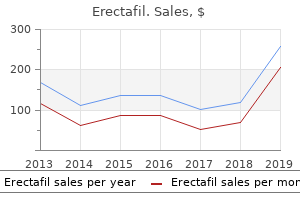
"Buy generic erectafil pills, erectile dysfunction medication free samples".
By: E. Carlos, M.B. B.CH., M.B.B.Ch., Ph.D.
Assistant Professor, Universidad Central del Caribe School of Medicine
This part of the larynx represents the narrowest portion of the respiratory system and is responsible for producing sound by audible vibration of the vocal folds latest advances in erectile dysfunction treatment buy cheap erectafil 20 mg. Posteriorly impotence beavis and butthead buy 20mg erectafil, where the vestibule ends, the stratified squamous epithelium becomes thinner and undergoes a transition to the pseudostratified epithelium that characterizes the respiratory region. It is lined by the respiratory mucosa that contains a ciliated, pseudostratified columnar epithelium on its surface. The underlying lamina propria is firmly attached to the periosteum and perichondrium of the adjacent bone or cartilage. The medial wall of the respiratory region, the nasal septum, is smooth, but the lateral walls are thrown into folds by the presence of three shelf-like, bony projections called conchae or turbinates. The conchae divide each nasal cavity into separate air chambers and play a dual role. They increase surface area and cause turbulence in airflow to allow more efficient conditioning of inspired air. The ciliated, pseudostratified columnar epithelium of the respiratory mucosa is composed of five cell types: the epithelium of the respiratory region of the nasal cavity is essentially the same as the epithelium lining most of the parts that follow in the conducting system. Because the respiratory epithelium of the trachea is studied and examined in preference to that of the nasal cavity, the above cell types are discussed in the section on the trachea (page 670). The arrangement of the vessels allows the inhaled air to be warmed by blood flowing through the part of the loop closest to the surface. The capillaries that reside near the surface are arranged in rows; the blood flows perpendicular to the airflow, much as one would find in a mechanical heatexchange system. These same vessels may become engorged and leaky during allergic reactions or viral infections such as the common cold. The lamina propria then becomes distended with fluid, resulting in marked swelling of the mucous membrane with consequent restriction of the air passage, making breathing difficult. Their secretions supplement that of the goblet cells in the respiratory epithelium. By increasing surface area, the conchae (turbinates) increase the efficiency with which the inspired air is warmed. The turbinates also increase the efficiency of filtration of inspired air through the process of turbulent precipitation. Particulate matter suspended in the air stream is thrown out of the stream and adheres to the mucus-covered wall of the nasal cavity. Particles trapped in this layer of mucus are transported to the pharynx by means of coordinated sweeping movements of cilia and are then swallowed. The lamina propria of the olfactory mucosa is directly contiguous with the periosteum of the underlying bone (Plate 69, page 688). This connective tissue contains numerous blood and lymphatic vessels, unmyelinated olfactory nerves, myelinated nerves, and olfactory glands. The olfactory epithelium, like the epithelium of the respiratory region, is also pseudostratified, but it contains very different cell types. In living tissue, this mucosa is distinguished by its slight yellowish brown color caused by pigment in the olfactory epithelium and the associated olfactory glands. Supporting or sustentacular cells are columnar cells that are similar to neuroglia cells and provide mechanical and metabolic support to the olfactory receptor cells. Basal cells are stem cells from which new olfactory receptor cells and supporting cells differentiate. This diagram shows the three major cell types located within the olfactory epithelium: the olfactory cell, supporting (sustentacular) cell, and basal cell. The olfactory cell is the receptor cell; it has an apical expansion, the olfactory vesicle, from which long, nonmotile cilia extend. At its basal surface, it extends an axon into the connective tissue that joins with axons of other olfactory cells to form an olfactory nerve.
The processes and the ciliary body are covered by a double layer of columnar epithelial cells erectile dysfunction papaverine injection discount erectafil 20 mg without prescription, the ciliary epithelium erectile dysfunction estrogen buy 20 mg erectafil otc, which was originally derived from the two layers of the optic cup. It can be caused by excessive secretion of aqueous humor or impedance of the drainage of aqueous humor from the anterior chamber. The internal tissues of the eye, particularly the retina, are nourished by the diffusion of oxygen and nutrients from the intraocular vessels. Blood flows normally through these vessels (including the capillaries and veins) when the hydrostatic pressure within the vessels exceeds the intraocular pressure. If the drainage of the aqueous humor is impeded, the intraocular pressure increases because the layers of the eye do not allow the wall to expand. This increased pressure interferes with normal retinal nourishment and function, causing the retinal nerve fiber layer to atrophy. The removal of aqueous humor is obstructed because of reduced flow through the trabecular meshwork of the iridocorneal angle into the scleral venous sinus (canal of Schlemm). Usually it is associated with a sudden, painful, complete blockage of the scleral venous sinus and can result in permanent blindness if not treated promptly. Visual deficits associated with glaucoma include blurring of vision and impaired dark adaptation (symptoms that indicate loss of normal retinal function) and halos around lights (a symptom indicating corneal endothelial damage). If the condition is not treated, the retina will be permanently damaged, and blindness will occur. Treatments are directed toward lowering the intraocular pressure by decreasing the rate of production of aqueous humor or eliminating the cause of the obstruction of normal drainage. Dorzolamide and brinzolamide are two carbonic anhydrase inhibitors that are currently available as eye drops to treat glaucoma. This image shows a view of the fundus of the left eye in a patient with advanced glaucoma. As a result of the increased intraocular pressure, retinal nerve fibers undergo atrophy and shrink in size. Note a pale optic disc in the center of the image with a less pronounced rim due to atrophy of nerve fibers. Enlargement of the optic nerve cup (central area of the optic disc) is also visible and a characteristic finding for glaucoma. The cell layer that has its basal lamina facing the connective tissue stroma of the ciliary body is heavily pigmented and is directly continuous with the pigmented epithelial layer of the retina. The double-layered ciliary epithelium continues over the iris, where it becomes the posterior pigmented epithelium and anterior pigmented myoepithelium. The zonular fibers extend from the basal lamina of the nonpigmented epithelial cells of the ciliary processes and insert into the lens capsule (the thickened basal lamina of the lens). The cells of the pigmented layer have a less developed junctional zone and often exhibit large, irregular lateral intercellular spaces. Both desmosomes and gap junctions hold together the apical surfaces of the two cell layers, creating discontinuous "luminal" spaces called ciliary channels. The aqueous humor is similar in ionic composition to plasma but contains less than 0. The main functions of the aqueous humor are to maintain intraocular pressure and to provide nutrients and remove metabolites from avascular tissues of the cornea and lens. The aqueous humor passes from the ciliary body toward the lens, and then between the iris and lens, before it reaches the anterior chamber of the eye. In the anterior chamber of the eye, the aqueous humor passes laterally to the angle formed between the cornea and iris. Here it penetrates the tissues of the limbus as it enters the labyrinthine spaces of trabecular meshwork and finally reaches the canal of Schlemm, which communicates with the veins of the sclera (see Folder 24. A potential space, the perichoroidal space (between the sclera and retina), is traversed by thin, ribbon-like, branching lamellae or strands that pass from the sclera to the choroid. These lamellae originate from the suprachoroid lamina (lamina fusca) and consist of large, flat melanocytes scattered between connective tissue elements, including collagen and elastic fibers, fibroblasts, macrophages, lymphocytes, plasma cells, and mast cells. The lamellae pass inward to surround the vessels in the remainder of the choroid layer. Free smooth muscle cells, not associated with blood vessels, are present in this tissue. Lymphatic channels called epichoroid lymph spaces, long and short posterior ciliary vessels, and nerves on their way to the front of the eye are also present in the suprachoroid lamina.
However erectile dysfunction what doctor to see buy discount erectafil 20 mg, these results were most likely due to the stannous ion rather than to fluoride; the positive charge of the stannous ion may interfere with bacterial membrane function erectile dysfunction medicine in dubai discount 20 mg erectafil with visa, bacterial adhesion, and glucose uptake, thereby inhibiting the formation of plaque. Prebrushing Rinses Essential Oils A mixture of essential oils consisting of thymol 0. Essential oils may reduce plaque levels by inhibiting bacterial enzymes and by reducing pathogenicity of plaque via reduction of the amount of endotoxin; the alcohol is probably responsible for denaturing bacterial cell walls. The substantivity of Listerine appears to be quite low, and therefore, it must be used at least twice a day to be effective. A variety of clinical studies have demonstrated that Listerine is capable of reducing plaque and gingivitis over extended periods; however, the degree of reduction is variable. Adverse reactions include a bitter taste and burning sensation in the oral cavity. Regular use of high-alcohol rinses can aggravate existing oral lesions and desiccate mucous membranes. The topical application of a liquid rinse before brushing as an aid in the mechanical removal of supragingival plaque is a novel idea. Since the introduction of the first prebrushing rinse there has been a rapid increase in the number of generic products that claim to physically loosen or remove plaque. Prebrushing rinses usually contain a plethora of ingredients, and it is not known which constituent is the active chemical. It has been suggested that sodium lauryl sulfate acts as a detergent to dislodge or loosen the plaque on teeth (Table 42. When prebrushing rinses were tested against placebo rinses, prebrushing rinses appeared to have no effect on plaque reduction. On an annual basis, Americans spend more than $750 million on oral rinsing agents, although few effective plaque-inhibiting oral rinses are available and many are associated with side effects that prohibit long-term use. The goal of future product development is not so much an improvement in the antiplaque performance of the existing effective compounds but rather lessening of their side effects and development of better delivery systems. Products that combine various known com- Fluorides Fluorides are widely used in caries prevention, for which they have been highly effective. Systemic administration of fluorides for caries prevention is available via drink- 42 Drugs for the Control of Supragingival Plaque 505 pounds with well-established plaque-inhibiting properties are under investigation. Among the most promising products are amine fluoride plus stannous fluoride and copper sulfate plus hexetidine. In the future, chemopre- vention of supragingival plaque will depend on products that are effective, substantive, and safe. The period during which a drug is in contact with a substrate in the oral cavity is (A) Excretion (B) Absorption (C) Distribution (D) Substantivity (E) Drug clearance 2. Yellow or brownish extrinsic stain of teeth is a frequently observed side effect of (A) Fluoride (B) Triclosan (C) Essential oils (D) Chlorhexidine (E) Sodium lauryl sulfate 3. Triclosan (A) is active against a broad range of oral gram-positive and gram-negative bacteria. Essential oils (B) are effective in reducing plaque levels by inhibiting bacterial enzymes. Chlorhexidine (C) is generally effective against all bacteria, but Streptococcus mutans and Actinomyces viscosus, two bacteria particularly associated with dental lesions, are especially susceptible to its action. Stannous fluoride (D) is widely used in caries prevention, and many studies have proven its effectiveness. None of the other compounds listed has been shown to decrease supragingival plaque in combination with the polymer in a commercial preparation. Excretion (A) and drug clearance (E) are factors involved in drug elimination, while absorption (B) describes the ability of a drug to cross membranes and enter the blood stream. Distribution (C) describes the ability of a drug to enter a variety of body compartments during its circulation in the blood. It is due to the ability of this cation to strongly bind to tooth surfaces, requiring strong abrasives to Addy M and Renton-Harper P.
The nerves enter the liver at the porta hepatis and ramify through the liver in the portal canals along with the members of the portal triad erectile dysfunction mental treatment buy generic erectafil. Sympathetic fibers innervate blood vessels erectile dysfunction leakage purchase erectafil 20 mg on-line, and increased stimulation in this system causes an increase of vascular resistance, decreased hepatic blood volume, and a rapid increase of serum levels of glucose. The parasympathetic fibers are assumed to innervate the large ducts (those that contain smooth muscle in their walls) and possibly blood vessels; their stimulation promotes glucose uptake and utilization. The cell bodies of parasympathetic neurons are often present near the porta hepatis. The gallbladder is a secondary derivative of the embryonic foregut, arising as an evagination of the primitive bile duct that connects the embryonic liver to the developing intestine. It is involved in the absorption of fat and is used by the liver as a vehicle for excretion of cholesterol, bilirubin, iron, and copper. The composition of bile and the specific functions of most of its components are listed in Table 18. As noted in the the gallbladder is a blind pouch that leads, via a neck, to the cystic duct. The gallbladder can store and remove about 90% of the water from the incoming bile, which results in an increase of bile salts, cholesterol, and bilirubin concentrations up to 10-fold. Hormones secreted by the enteroendocrine cells of the small intestine, in response to the presence of fat in the proximal duodenum, stimulate contractions of the smooth muscle of the gallbladder. Because of these contractions, concentrated bile is discharged into the common bile duct, which carries it to the duodenum. The lamina propria of the mucosa is particularly rich in fenestrated capillaries and small venules, but there are no lymphatic vessels in this layer. The lamina propria is also very cellular, containing large numbers of lymphocytes and plasma cells. The characteristics of the lamina propria resemble those of the colon, another organ specialized for the absorption of electrolytes and water. Mucin-secreting glands are sometimes present in the lamina propria in the normal human gallbladder, especially near the neck of the organ, but they are more commonly found in inflamed gallbladders. Cells that appear identical to enteroendocrine cells of the intestine are also found in these glands. External to the lamina propria is a muscularis externa that has numerous collagen and elastic fibers among the bundles of smooth muscle cells. Despite its origin from a foregutderived tube, the gallbladder does not have a muscularis mucosae or submucosa. The mucosa of the gallbladder consists of a lining of simple columnar epithelial cells and a lamina propria of loose connective tissue, which typically exhibits numerous deep folds in the mucosa. External to the muscle is an adventitia containing adipose tissue and blood vessels. The portion of the gallbladder not attached to the liver displays a typical serosa instead of an adventitia. The tall columnar cells display features typical of absorptive cells, with microvilli on their apical surface, an apical junctional complex separating the lumen of the gallbladder from the lateral intercellular space, and numerous mitochondria in the apical portion of the cell. During active fluid transport, salt is pumped from the cytoplasm into the intercellular space, and water follows the salt. As this process continues, the intercellular space becomes greatly distended (arrows). The increase in size of the lateral intercellular space during active fluid transport is evident with the light microscope. Contraction of the smooth muscle reduces the volume of the bladder, forcing its contents out through the cystic duct. This layer contains large blood vessels, an extensive lymphatic network, and the autonomic nerves that innervate the muscularis externa and the blood vessels (cell bodies of parasympathetic neurons are found in the wall of the cystic duct). The layer of tissue where the gallbladder attaches to the liver surface is referred to as the adventitia.
If there are associated seizures with no other attributable cause erectile dysfunction definition discount erectafil 20mg otc, this is eclampsia erectile dysfunction video order erectafil 20 mg mastercard. More than 30% of seizures occur postnatally, so women developing pre-eclampsia in the antenatal period also require close postnatal surveillance. It certainly has a genetic component with significantly increased risk in firstdegree relatives. The primary pathology seems to be placental in nature, with poor placentation in the first and second trimesters leading to placental ischaemia. There is a maternal inflammatory response with endothelial dysfunction, increased capillary permeability, and microvascular vasoconstriction. It is important to remember that some of these symptoms are common in pregnancy and may have other causes; however, a high index of suspicion should always be maintained. Investigations In addition to quantifying the urinary protein, the following investigations may be helpful. Supportive treatment Management of pre-eclampsia the definitive cure for pre-eclampsia is delivery of the fetus and placenta. The challenge involves balancing the risks of continuation of the pregnancy to both the mother and the fetus against the risks of prematurity to the fetus. Ultimately maternal well-being supersedes fetal rights, and in very severe cases delivery may be warranted with the knowledge that the fetus is non-viable. Once the diagnosis of pre-eclampsia is made, an assessment of the severity of the disease must be carried out. If the pre-eclampsia is felt to be mild, then a senior clinician may consider allowing careful out-patient management, with frequent surveillance via day assessment units; however, in most cases the diagnosis of pre-eclampsia warrants in-patient care. Fluid balance: in severe pre-eclampsia; to reduce the risk of pulmonary oedema reduce fluid intake to 80 mL/hour and monitor urine output; invasive monitoring may be required. Corticosteroids for fetal lung maturation If pre-term and delivery is anticipated within 7 days. If there is concurrent fetal growth restriction, particularly in the presence of abnormal fetal Dopplers, then delivery by caesarean section may be preferred, If attempting vaginal delivery, then continuous fetal heart rate monitoring should be in place. Unless the blood pressure is very poorly controlled, there is no need to limit the second stage of labour. It is characterised by: Blood pressure control Pharmacological treatment is warranted if the blood pressure is greater than 150/100 mmHg. If systolic blood pressure is >160 mmHg there is significantly increased risk of stroke. Hydralizine can be used if blood pressure is very high but use with care as it can cause acute hypotension. Prevention of pre-eclampsia All women should be risk assessed at their booking appointment as to their likelihood of developing pre-eclampsia. If they have one high-risk factor or two or more moderate risk factors, then they should be started on low-dose aspirin (75 mg), as this is only measure that has been shown to improve outcome. Since these conditions can lead to rapid maternal deterioration, accurate diagnosis and early treatment is essential. Acute fatty liver of pregnancy Patients present, generally in the third trimester, with non-specific symptoms such as nausea, vomiting, headache, malaise, or abdominal pain. Physical and laboratory findings may include jaundice, hypertension, hypoglycaemia, hyperbilirubinaemia, coagulopathy, elevated creatinine, and elevated transaminases. The results of this will allow further risk assessment as to how likely the mother is to develop pre-eclampsia and how likely the fetus is to develop growth restriction. Hypertension is common in association with renal dysfunction, making distinguishing it from pre-eclampsia difficult in early gestations. Evidence of dermatologic (malar or discoid rash) and arthritic complaints in conjunction with the other clinical findings, as well as an atypical presentation for pre-eclampsia, will commonly suggest this alternative diagnosis.
The external and middle ear collect and conduct sound energy to the internal ear erectile dysfunction what age does it start order erectafil overnight delivery, where auditory sensory receptors convert that energy into electrical impulses erectile dysfunction surgery options best 20 mg erectafil. The sensory receptors of the vestibular system respond to gravity and movement of the head. They are responsible for the sense of balance and equilibrium and help to coordinate movements of the head and eyes. The ear develops from surface ectoderm and components of the first and second pharyngeal arch. The malleus and incus develop from the first pharyngeal arch, and the stapes from the second pharyngeal arch. The auricle of the external ear develops from six auricular hillocks located at dorsal ends of the first and second pharyngeal arches surrounding the first pharyngeal cleft. The cartilaginous, bony, and muscular structures of the ear develop from the mesenchyme surrounding these early epithelia. Embryologically, the functions of the ear-hearing and balance-are elaborated from an invagination of surface ectoderm that appears on each side of the myelencephalon. This invagination forms the otic vesicle (otocyst), which sinks deep to the surface ectoderm into the underlying mesenchyme. The otic vesicle serves as a primordium for development of the epithelia that line the membranous labyrinth of the internal ear. Later, development of the first and part of the second pharyngeal arch provides structures that augment hearing. The endodermal component of the first pouch gives rise to the tubotympanic recess, which ultimately develops into the auditory tube (Eustachian tube) and the middle ear and its epithelial lining. The corresponding ectodermal outgrowth of the first pharyngeal groove gives rise to the external acoustic meatus and its epithelial lining. The connective tissue part the auricle (pinna) is the oval appendage that projects from the lateral surface of the head. The characteristic shape of the auricle is determined by an internal supporting structure of elastic cartilage. Thin skin with hair follicles, sweat glands, and sebaceous glands cover the auricle. The auricle is considered a nearly vestigial structure in humans, compared with its development and role in other animals. The external acoustic meatus is an air-filled tubular space that follows a slightly S-shaped course for about 25 mm to the tympanic membrane (eardrum). The three divisions of the ear are represented by different colors and consist of the external ear (auricle and external acoustic meatus; pink tone), the middle ear (tympanic cavity, auditory ossicles, tympanic membrane, and auditory tube; green), and the internal ear containing the bony labyrinth (semicircular canals, vestibule, and cochlea; blue) and the membranous labyrinth (not visible). Both parts of the meatus are lined by skin, which is also continuous with that of the auricle. The skin in the lateral part of the meatus contains hair follicles, sebaceous glands, and ceruminous glands but no eccrine sweat glands. The coiled tubular ceruminous glands closely resemble the apocrine glands found in the axillary region. Their secretion mixes with that of the sebaceous glands and desquamated cells to form cerumen, or earwax. Because the external acoustic meatus is the only blind pouch of the skin in the body, the earwax provides the means to evacuate desquamating cells from the stratum corneum, thus preventing their accumulation in the meatus. The cerumen lubricates the skin and coats the meatal hairs to impede the entry of foreign particles into the ear. Excessive accumulation of cerumen (impacted cerumen) can plug the meatus, resulting in conductive hearing loss. The medial part of the meatus located within the temporal bone has thinner skin and fewer hairs and glands. The tympanic cavity has a roof, floor, and four walls: anterior, posterior, lateral, and medial. The tympanic cavity contains an opening of the auditory tube and is bound anteriorly by a thin layer of bone that separates it from the internal carotid artery. The posterior wall of the tympanic cavity is formed by the spongy bone of the mastoid process, which contains the mastoid antrum and other, smaller air-filled spaces called mastoid air cells. The middle ear is bound laterally by the tympanic membrane and medially by the bony wall of the internal ear.
Diseases
- Metaphyseal dysplasia maxillary hypoplasia brachydactyly
- Hyperaldosteronism familial type 2
- Rectosigmoid neoplasm
- Spinal shock
- Mediastinal syndrome
- Fox Fordyce disease
- Katz syndrome
- Pierre Robin sequence congenital heart defect talipes
- Hamano Tsukamoto syndrome
- Vitamn B6 deficiency
In humans erectile dysfunction hypertension order generic erectafil canada, it is likely that the capillaries first perfuse the A and D cells impotence kidney stones order discount erectafil on line, peripherally, before the blood reaches the B cells, centrally. Larger vessels that travel in septa that penetrate the central portion of the islet are also accompanied by A and D cells, so that blood reaching the B cells has always first perfused the A and D cells. Recent in vivo fluorescence imaging studies show distinct blood flow dynamics in the islets of Langerhans. These studies suggest that blood flow is regulated by the blood glucose levels in addition to the complex interaction among vasodilators and vasoconstrictors, gastrointestinal peptides, and the autonomic nervous system. Large efferent capillaries leave the islet and branch into the capillary networks that surround the acini of the exocrine pancreas. This cascading flow resembles the portal systems of other endocrine glands (pituitary, adrenal). It is a small protein consisting of two polypeptide chains joined by disulfide bridges. Its biosynthesis presents a clear example of the importance of posttranslational processing in the achievement of the final, active structure of a protein. Posttranslational processing reduces the preproinsulin to a polypeptide with a molecular weight of about 9,000 Da. Proinsulin is a single polypeptide chain of 81 to 86 amino acids that has the approximate shape of the letter G. It is stored in the secretory vesicles and released with the insulin in equimolar amounts. Because C peptide has a longer half-life than insulin, higher concentrations of C peptides are detected in the peripheral blood. For these reasons, measurement of circulating levels of C peptides provides important clinical information about the secretory activity of B cells. Because C peptide is cleared from the body by the kidney, measurement of its urinary excretion provides useful information about B-cell insulin secretion. C peptide measurements are frequently used to assess the residual B-cell function in patients treated with insulin, to distinguish between types 1 and 2 diabetes, and in the diagnosis and monitoring therapy of insulinoma (tumor of B cells). C peptide may also be used to monitor the progress of pancreas or islet cell transplantation. Insulin is synthesized as the preproinsulin, a single polypeptide chain that undergoes posttranslational modifications. The liver plays an important role in the uptake, storage, and distribution of nutrients. The liver also acts as an exocrine organ (produces bile) and performs endocrine-like functions. The liver has a dual blood supply: a venous supply via the hepatic portal vein and an arterial supply via the hepatic artery. Hepatocytes (as seen in the classic lobule) are organized into irregular anastomosing plates that radiate toward a central vein. Corners of the polygonal classic lobule are occupied by the portal triad, which contains branches of portal vein, hepatic artery, bile ducts, and small lymphatic vessels. Hepatic sinusoids form irregular vascular channels that run parallel and between the plates of hepatocytes. They receive mixed blood (75%) from venous portal circulation and arterial blood (25%) from systemic circulation. The perisinusoidal space (space of Disse) lies between hepatocytes and the endothelium; it is the site of exchange of materials between blood and liver cells. The sinusoidal endothelium includes specialized stellate sinusoidal macrophages (Kupffer cells), which remove senile red blood cells and recycle iron molecules. Hepatic stellate cells (Ito cells) reside in perisinusoidal spaces and are loaded with lipid droplets for storage of vitamin A. In pathologic conditions, Ito cells have the potential to differentiate into myofibroblasts. The basal surface of hepatocytes has contact with the perisinusoidal space (of Disse), whereas the apical surface is connected to the adjacent hepatocyte to form a bile canaliculus. Bile canaliculi drain into the short canals of Hering, which are partially lined by hepatocytes and cuboidal cholangiocytes (cells lining the biliary tree).
Pathological Fetal bradycardia A baseline fetal heart rate of less than 110 bpm is considered a fetal bradycardia impotence lexapro buy erectafil 20mg without a prescription. It can be physiological in the postterm fetus as a result of continuing development of the vagus erectile dysfunction self treatment cheap erectafil 20 mg on-line. Pathological Box 3 Causes of reduced fetal baseline variability Physiological Quiet sleep state Narcotics. A sustained fetal bradycardia is an obstetric emergency, and such causes as placental abruption, uterine rupture, uterine hyperstimulation, and cord prolapse must be considered. Pathological Reduced baseline variability A reduced baseline variability is less than 5 bpm. It is a non-reassuring baseline if it lasts for more than 40 but less than 90 minutes. If the reduced baseline variability lasts for more than 90 minutes, it is abnormal (see Table 2). The presence of normal baseline variability requires an intact cerebral cortex, midbrain, vagus nerve, and a cardiac conduction system. A normal baseline variability indicates that the fetus does not suffer from cerebral asphyxia. A gradual reduction of the baseline variability in the presence of other patterns of fetal hypoxia indicates that the fetal compensatory mechanism to maintain cerebral oxygenation is being lost. Sinusoidal patter A regular oscillation of the baseline long-term variability that resembles a sine wave is called a sinusoidal pattern. The pattern was first described in infants with severe rhesus alloimmunisation and fetal anaemia. Uterine activity needs to be monitored accurately in order to classify the different decelerations, as management would depend on the type of the deceleration. In the presence of a nonaccelerative trace with baseline variability <5 bpm, the definition would include decelerations <15 bpm. Late decelerations are thought to be caused by a decreased blood flow (associated with a uterine contraction) beyond the capacity of the fetus to extract oxygen. Atypical variable deceleration In addition to the features described, variable decelerations are said to be atypical if they have any of the following characteristics. True early uniform decelerations are rare and benign, and therefore they are not significant. If a bradycardia occurs in the baby for more than 3 minutes, urgent medical aid should be sought and preparations should be made to urgently expedite the birth of the baby, classified as a category 1 delivery. This could include moving the woman to theatre if the fetal heart has not recovered by 9 minutes. If the fetal heart recovers within 9 minutes, the decision to deliver should be reconsidered in conjunction with the woman if appropriate. However, an increase in the baseline heart rate, even within the normal range, with other non-reassuring or abnormal features should increase concern about the well being of the fetus. It is therefore important to ensure that both types of variable decelerations, especially atypical ones, are recognised and that appropriate action is taken. If a third sample is required, a consultant should be involved in further decisions about the labour. The history must be interpreted with reference to the gestational age, as aetiologies change throughout pregnancy. Specific questions that may aid diagnosis include: Did the pain start gradually or suddenly Routine electronic monitoring of fetal heart rate and uterine activity during labor. Fetal heart rate monitoring during labour: too frequent intervention, too little benefit Peritoneal signs are often absent in pregnancy as a result of lifting and stretching of the anterior abdominal wall. This means that any underlying inflammation is not in direct contact with the peritoneum, thus reducing guarding. It may be useful to examine the patient in the lateral decubitus position to help distinguish between uterine and extrauterine pain.
Severe sepsis this occurs when in a patient with sepsis and symptoms and signs of organ dysfunction erectile dysfunction treatment pune erectafil 20mg with visa, as described in Table 1 erectile dysfunction in diabetes mellitus pdf generic 20mg erectafil free shipping. Septic shock If the hypotension or raised lactate does not respond to fluid resuscitation, the patient is in septic shock. Acute appendicitis-like symptoms as initial presentation of ovarian vein thrombosis. Vulvovaginal haematoma complicating delivery: rationale for drainage of the haematoma cavity. Risk factors for fever, endometritis and wound infection after abdominal delivery. Bacteriuria in the puerperium: risk factors, screening procedures, and treatment programs. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Eclamptic seizures are almost always self-limiting, with a usual duration of 60 to 75 seconds (seldom longer than three to four minutes). It can occur anytime from the 2nd trimester to the puerperium (see Collapse in pregnancy). In a convulsion, the body muscles contract and relax rapidly and repeatedly, resulting in uncontrollable shaking. In developing countries, however, the incidence varies widely from 6 to 157 per 10,000 deliveries. The following two hypotheses have been proposed: Causes the causes of fits in pregnancy can be divided into obstetric and non-obstetric: Obstetric eclampsia; postdural puncture. Cerebral overregulation in response to high systemic blood pressure results in vasospasm of cerebral arteries, under perfusion of the brain, localised ischaemia/infarction, and cytotoxic (intracellular) oedema. Loss of auto-regulation of cerebral blood flow in response to high systemic pressure. Features of severe pre-eclampsia which may occur before the seizure1,4,5,8,9 Eclampsia Eclampsia is a convulsive condition associated with pre-eclampsia. It is a clinical diagnosis based on Severe headache, persistent frontal or occipital headache, headache that persists and progresses despite analgesic therapy. Systolic blood pressure 160 mmHg or diastolic blood pressure 110 mmHg on two occasions at least four hours apart while the patient is on bed rest. However, brain damage from haemorrhage or ischemia may result in permanent neurological problems and is the most common cause of death in eclamptic women. The highest rates are in developing countries where prenatal, intrapartum, and neonatal care are compromised by limited resources. Effect on fetus 4,5,11,12 Short fetal bradycardia for a few minutes is a common finding during and immediately after an eclamptic seizure, and emergency caesarean delivery is not always necessary. Stabilising the mother by administering anti-convulsant drugs, oxygen, and antihypertensive drugs can help the fetus recover in utero. Resolution of maternal seizure activity is associated with a compensatory fetal tachycardia and loss of variability, sometimes associated with transient fetal heart rate decelerations. If the fetal heart rate tracing remains non-reassuring for more than 10 or 15 minutes with no improvement despite maternal and fetal resuscitations, then the possibility of an occult abruption should be considered and emergency delivery may be indicated. Premature delivery, abruptio placenta, and intrauterine asphyxia are the primary causes of perinatal death in eclamptic pregnancies. Perinatal mortality ranges from 2 to 23 per cent and is closely related to gestational age. In addition, there is a two- to three-fold increased risk of delivery of a small-for-gestationalage infant. Non-white, nulliparous women from lower socioeconomic backgrounds are the group at highest risk of developing eclampsia.
The primary problem is a non-specific inflammatory condition labelled periductal mastitis erectile dysfunction at the age of 17 20 mg erectafil amex, which can be complicated by secondary bacterial infection and enlargement impotence thesaurus generic erectafil 20mg line, or ectasia, of ducts. The condition is seen typically in women in their 30s and 40s, and there is an association with smoking. The discharge is from multiple ducts, usually bilateral, can be of various colours, and, on occasions, be tinged with blood. Some of the women with this problem may have nipple inversion as a consequence, or a possible cause, of the problem. Rarely, a fistula will develop, or occur following a procedure to drain an abscess, between a duct and an opening on the areola, or beyond. There are other simple, non-cardiac, causes for shortness of breath in pregnant women, such as iron deficiency anaemia and exacerbation of underlying respiratory conditions. The usual presentation is of an unhealed ulcer, the erosive lesion not having been noticed, and in some cases the complaint may be of a slight discharge, with or without blood. Cardiomyopathies and congenital heart disease constitute two of the main life-threatening conditions for the mother and her baby1,2. Cardiomyopathies Cardiomyopathy in pregnancy mainly comprises three types: peripartum, dilated, and hypertrophic. It is rare, but with great geographical variation in incidence (from 1:300 to 1:4000 pregnancies). Predisposing factors appear to be family history of the disease, multiparity, multiple child births, teen pregnancy or advanced age of mother, ethnicity, smoking, diabetes, hypertension, preeclampsia, and prolonged use of beta-blockers. Data for prognosis in Europe is sparse, but worldwide prognosis appears to vary geographically. Between 20 and 40 per cent of women return to normal cardiac function, although mortality can be as high as 28 per cent after 2 years. Further work has focussed on the anti-angiogenic effect of the postpartum placenta. Symptoms of breathlessness, orthopnoea, and paroxysmal nocturnal dyspnoea, along with abdominal pain from hepatic congestion, dizziness, and palpitations, usually develop in the 4 months after delivery, although 10 per cent may present in the final month of gravidum. Clinical signs may vary, but are usually consistent with congestive cardiac failure. Treatment of heart failure after delivery should follow usual therapeutic guidelines. Pharmacological management during pregnancy should take into account recommendations for avoiding fetal harm. Women with a murmur and an increased gradient across the left ventricular outflow tract may present for the first time in pregnancy. Maternal death is uncommon, and there is no evidence to suggest the risk of sudden death is increased by pregnancy. Women with severe diastolic dysfunction may be at risk of pulmonary congestion or even florid pulmonary oedema. Beta-blockers should be continued and a small dose of diuretic may help, but rest is recommended in conjunction with the beta-blocker in order to prevent tachycardia. Cardioversion may be considered if rate control fails, after excluding thrombus in the left atrial appendage with a transoesophageal echocardiogram. Finally, the genetic risk should be discussed, including the phenomenon of anticipation, which determines an earlier onset and more severe form in succeeding generations in some families. Normal vaginal delivery with good analgesia and a low threshold for forceps assistance is the safest mode of delivery for the mother with any form of cardiomyopathy, since it is associated with reduced blood loss and less rapid haemodynamic changes in comparison with caesarean section. Some have simple defects, such as small atrial or ventricular septal defects that may remain clinically silent until diagnosed on routine examination, whereas others have complex abnormalities that require surgical intervention for survival. Advances in cardiology and cardiac surgery have led to more than 85 per cent of these infants surviving into childbearing age, and the number is growing by approximately 1600 new cases every year. These women are at heightened risk of maternal and fetal complications should they conceive. The medical profession should, therefore, be aware of the clinical presentations, diagnosis, and management of the following conditions.