Cheap 100mcg rhinocort free shipping
Antegrade fluoroscopic venography usually fills extensive collaterals around the obstruction allergy treatment bangalore purchase rhinocort toronto, but also often highlights the true lumen as a thin allergy forecast ontario safe rhinocort 200mcg, straight channel (the socalled "string sign"). In these scenarios, the catheter should be retracted by the operator and recannulation of the true channel attempted. The goal is that the wire either crosses the obstruction independently or sheaths become positioned in "dead space" adjacent to one another. Sharp recanalization/loop snare technique can then be used or side-by-side balloon angioplasty performed to unite the lumens. Once the authors have crossed the obstruction, they confirm a safe track before large balloon dilation. The latter is particularly useful because it also provides anatomic relationships with nearby critical structures, for instance, the right renal or iliac arteries. After the operator deems the track safe, anticoagulation is initiated before sequential balloon dilation. The authors begin with the 8-mm balloon dilation of an iliocaval segment followed by contrast injection to exclude extravasation. If the estimated stent size is too small for the iliac veins, then the authors choose an appropriate stent size that allows for complete stent-wall apposition. Just as in the arterial system, long-term stent patency relies on adequate inflow and outflow. Venography of the femoral and deep femoral veins is performed to assess inflow before case completion. The desired anastomotic site on the popliteal vein is exposed, and the vein segment is isolated with silicone elastomer vessel loops. Before completing the anastomosis, the segment is back-bled and forward-bled to prevent embolization of air or debris. A side-biting clamp is applied to the popliteal artery distal to the saphenopopliteal anastomosis. The arteriovenous anastomosis is then completed in an end-to-side manner with 6-0 polypropylene suture. A side-biting vascular clamp is then applied to the popliteal vein and a venotomy is created. Size and positioning of the interposition graft are crucial to achieve success with future embolization. After dressing the wound, a compression wrap is applied while the patient remains in the operating room. The authors encourage early ambulation, the use of elastic compression wraps or stockings and, while hospitalized, the use of intermittent pneumatic compression to encourage flow through the reconstruction. The bilateral lower extremities are prepped circumferentially, as well as the abdomen. Again, the presence of a unilateral iliac vein occlusion can result in extensive cross-pubic collateral veins. The suprapubic tunnel should be made very carefully to prevent disruption of the collateral system. The bilateral groin incisions are then closed in a layered fashion, with a surgical drain secured in each wound. Postoperatively, patients are started on low-molecularweight heparin or oral anticoagulation. Again, the authors encourage early ambulation, the use of elastic compression wraps or stockings and, while hospitalized, the use of intermittent pneumatic compression. Alternatively, tangential aneurysmectomy and lateral venorrhaphy can be performed. The patient is then transported to the operating room, where general anesthesia is induced and the patient is placed prone on the operating room table.
Discount 200 mcg rhinocort with mastercard
Glucocorticoid Suppression of Adrenal Function A highly significant aspect of long-term therapy with exogenous pharmacologic preparations of the glucocorticoids allergy testing yorkville toronto purchase cheap rhinocort on-line. Chronic suppression causes atrophy of the adrenal gland allergy air purifier rhinocort 100 mcg, and the abrupt withdrawal of glucocorticoids in exogenous or endogenous causes can result Glenn Matfin in acute adrenal insufficiency especially during periods of stress or when surgery is performed. Recovery to a state of normal adrenal function may be prolonged, requiring up to 12 months or more (28). Clinical Assessment It is crucial to recognize clinical features suggestive of adrenal insufficiency, because if present, they identify symptomatic patients who may require urgent corrective measures. The severity of signs and symptoms depends both on the absolute degree of glucocorticoid and mineralocorticoid deficiency and the rapidity of its onset. In comparison, patients with chronic adrenal insufficiency can have more insidious presentation. It is important to ask patients, relatives or health care providers about any relevant history, including any exposure to steroid therapy in any formulation, including over-thecounter agents. Hyperpigmentation occurs in more than 90% of persons with Addison disease, and is helpful in distinguishing the primary and secondary forms of adrenal insufficiency (Tables 20-1 and 20-2). Except for salt craving, the symptoms of primary adrenal insufficiency are rather nonspecific and include weakness, fatigue; musculoskeletal pain and cramps; weight loss, abdominal pain, nausea and vomiting; depression, and anxiety. As a result, the diagnosis is frequently delayed, resulting in a clinical presentation with an acute life-threatening adrenal crisis (which is the presentation in more than half of patients with adrenal insufficiency). Secondary Adrenal Insufficiency Central hypoadrenalism may lead to dehydration, hyponatremia (due to dilution and not mineralocorticoid deficiency) and shock, unresponsive to fluid resuscitation and vasopressor therapy before glucocorticoid replacement is administered. Patients with central hypoadrenalism may present with prostration, headache, nausea, vomiting, orthostatic dizziness, joint and muscle aches, dehydration, confusion, shock, and hyponatremia (6). Patients with disease of long duration may additionally report fatigue and unexplained weight loss. Indications of empirical glucocorticoid treatment are hemodynamic instability, altered consciousness level, reduced visual acuity or severe visual field defects. Diagnostic Testing of Adrenal Insufficiency the increased requirements for cortisol during physiological stress make it crucially important not to miss a diagnosis of adrenal insufficiency in acute and critically ill patients. However, diagnostic measures should never delay prompt treatment of suspected adrenal crisis. Preferably, a stimulated cortisol is evaluated for investigation of adrenal hypofunction. However, assays cross-react differently with cortisol, and the target and threshold values are assay-dependent and local normal ranges should be used. Another variation of the cosyntropin or synacthen test uses a low-dose 1 g for adrenal stimulation. Primary Adrenal Insufficiency the 2016 Endocrine Society Clinical Practice Guideline (5) recommended diagnostic testing for the exclusion of primary adrenal insufficiency in acutely ill patients with otherwise unexplained indicative clinical symptoms or signs. This is also recommended for pregnant women with unexplained persistent nausea, fatigue, and hypotension. Peak cortisol levels below 500 nmol/L (18 g/dL) (assay dependent) at 30 or 60 minutes indicate adrenal insufficiency. The simultaneous measurement of plasma renin and aldosterone in primary adrenal insufficiency is also indicated to determine the presence of mineralocorticoid deficiency. Morning cortisol <140 nmol/L (5 g/dL) is suggestive of adrenal insufficiency (and needs confirmatory testing). Measuring plasma corticotropin levels in a concurrent specimen may help to distinguish between central hypoadrenalism (characterized by low or "normal" plasma corticotropin) and primary adrenal insufficiency (characterized by elevated plasma corticotropin). Young males and males without autoantibodies should be screened for adrenoleukodystrophy by measuring very-long chain fatty acids (25). Genetic diseases should also be investigated (after appropriate genetic counselling) as indicated. These etiologies can be screened for using 21-hydroxylase antibodies and a baseline serum 17-hydroxyprogesterone level. The latter includes subtypes of autoimmune polyglandular syndromes or specific rare genetic disorders where adrenal failure is part of a broader phenotype.
Buy rhinocort 100 mcg on line
Vitamin supplementation allergy forecast boston rhinocort 100mcg without a prescription, particularly thiamine allergy treatment emergency order 100mcg rhinocort visa, should be given intravenously to replace any possible coexisting deficiency. Cardiovascular complications including atrial dysrhythmia and congestive heart failure are treated with conventional means including antiarrhythmic agents, vasodilators, and diuretics. Congestive heart failure occurs largely as a result of impaired myocardial contractility and is aggravated by atrial dysrhythmia, particularly fibrillation. Strong consideration should be given to Swan-Ganz monitoring of central hemodynamics in these patients, since despite modern critical care advances, management of heart failure in thyroid storm continues to prove difficult. With each medication used, careful examination of its effects on thyroid hormones is required to avoid exacerbation of thyrotoxicosis. Beta-blockers are a mainstay of therapy, but there are several special considerations. Propranolol is contraindicated in patients with a history of asthma or chronic obstructive pulmonary disease, who should be considered for other agents such as calcium channel blockers, 1-selective beta-blockers, or reserpine. Propranolol has also been associated with cases of cardiorespiratory arrest in thyroid storm patients (72) further justifying the use of an intensive care setting. While propranolol has been the betablocker of choice for many decades (because of its additional benefit of peripheral Alicia L. Esmolol has definite utility over propranolol depending on the clinical circumstance. Calcium-channel blockers used for atrial fibrillation can potentially lead to dramatic falls in systemic vascular resistance and consequent severe hypotension (78). In regards to digoxin, somewhat larger loading and maintenance doses may be required in thyrotoxic patients, owing, presumably, to an increased distribution space and/or rapid metabolism of this drug (78). Serum digoxin levels should be closely monitored, particularly as thyrotoxicosis improves, to prevent digitalis toxicity. The empiric use of glucocorticoids in the treatment of thyroid storm was begun in the 1950s in an attempt to address the accelerated release and turnover of corticosteroids in thyroid storm (1). Indeed, inappropriately normal (rather than elevated) levels of serum cortisol have been observed in thyroid storm compared to other periods of significant stress (14). In addition to these effects, glucocorticoids such as dexamethasone and hydrocortisone have inhibitory effects on the peripheral conversion of T4 to T3. Further, the use of these agents appears to have led to improved survival in thyroid storm (7,14). The dose may be subsequently reduced and discontinued as allowed by the clinical response of the individual patient. Measures Directed against Precipitating Events in Thyroid Storm Although the event precipitating thyroid storm may be quite obvious, such as surgery, labor (79), withdrawal of thionamides (12), or recent use of radioiodine (80), this is frequently not the case. The fever and leukocytosis found in thyroid storm even in the absence of an infection may be difficult to distinguish from an occult infectious process (81). A careful culturing of blood, sputum, and urine is therefore indicated in the febrile thyrotoxic patient. The routine use of broad spectrum antibiotics is, however, not recommended in the absence of other evidence suggestive of infection. In cases of thyroid storm precipitated by hypoglycemia, diabetic ketoacidosis, stroke, or pulmonary embolism, standard therapeutic approaches apply and should be instituted simultaneously with the treatment of thyroid storm. In the stuporous or comatose patient who is unable to provide a history suggestive of a particular precipitating event, a high index of suspicion for these varied etiologies must be maintained. It should be remembered that in some individuals no precipitant will be identified, even in retrospect. After the Storm: Definitive Treatment For the patient successfully treated during the acute stages of thyroid storm, a key objective should be the prevention of a recurrent crisis by planning for definitive therapy with either radioactive iodine ablation or surgery. As the severely thyrotoxic patient improves clinically, a gradual withdrawal of treatment modalities is often Life-Threatening Thyrotoxicosis possible. Corticosteroids should be gradually tapered and discontinued, while -blockade, unless contraindicated, should generally be continued during this period.
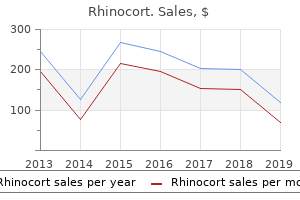
| Comparative prices of Rhinocort |
| # | Retailer | Average price |
| 1 | Office Depot | 313 |
| 2 | Subway | 766 |
| 3 | Winn-Dixie Stores | 410 |
| 4 | Stater Bros. Holdings | 636 |
| 5 | Darden Restaurants | 923 |
Order rhinocort overnight
Postoperative venous thromboembolic prophylaxis is maintained both mechanically (intermittent pneumatic compression) and pharmacologically (subcutaneous heparin) allergy symptoms to shellfish order 200mcg rhinocort with mastercard. Overall allergy partners asheville nc cheap 200mcg rhinocort visa, recent series reported late mortality to compare favorably with the other methods of reconstruction. If available, a second surgical team to harvest the femoral veins can help ameliorate this. Another disadvantage is the size mismatch between the infrarenal aorta, particularly when the initial operation was for aneurysmal disease, and the proximal end of the graft even when a bifurcated vein graft is created. In cases of an unstable patient from hemorrhage or sepsis, an alternative conduit should be considered. Finally, postoperative venous complications, including disruption of venous drainage with subsequent leg swelling, deep vein thrombosis, and compartment syndrome with need for fasciotomy have been reported. This approach avoids placement of a prosthetic graft in an infected field, as well as the time and morbidity associated with femoral vein harvest. Current cryopreservation techniques have improved the integrity of these grafts leading to fewer Case example 317 long-term complications than have been reported in the past. The downside to their use includes cost, and the lead time necessary for their acquisition. Thus, cryopreserved allografts may not be an option in an urgent or emergent situation. Once thawed, it is sewn in place in the standard fashion with the one caveat that the lumbar branches are placed facing up, to allow for ease of repair if there is any bleeding once the allograft is pressurized. At 5 years, freedom from graft-related complications was 80%, freedom from graft explant 88%, and freedom from limb loss 97%. Some need longer courses; occasionally, lifelong oral suppressive antibiotics are used. A variety of reconstructive options are available, but all depend on the administration of culture-specific antibiotics, aggressive debridement of all infected tissue, and maintenance of vital organ and limb perfusion. Currently available Dacron grafts pretreated with gelatin can be easily impregnated with an antibiotic when soaked in rifampin. Advantages of using antibiotic-treated prosthetic grafts include having a readily available, appropriately sized graft. As with other in-line arterial reconstructions, it avoids aortic stump blowout complications and has superior graft patency compared to extra-anatomic bypass. Like other in situ reconstructions, limb loss is rare and 5-year survival is around 50%. Reinfection is encountered more frequently with virulent organisms, particularly methicillin-resistant S. Radical debridement of the affected retroperitoneal tissue and use of an omental wrap are important adjuncts to reduce reinfection rates. When femoral artery anastomoses are involved, open groin wounds frequently result and are best managed with negative-pressure wound therapy. A graft enteric fistula was identified; this required resection of the small bowel and primary anastomosis. Antibiotic therapy of aortic graft infection: treatment and prevention recommendations. Aortic graft infections: is there still a role for axillobifemoral reconstruction Reinfection after resection and revascularization of infected infrarenal abdominal aortic grafts. Use and durability of femoral vein for autologous reconstruction with infection of the aortoiliofemoral axis. The use of cryopreserved aortoiliac allograft for aortic reconstruction in the United States.
Buy rhinocort cheap
In other words gluten allergy symptoms quiz generic rhinocort 100mcg without prescription, how society defines drug abuse determines how society responds to drug use allergy forecast corpus christi discount rhinocort 100mcg line. The traditional way of considering the question of drug use and crime is the tripartite model offered by Paul Goldstein (1985): 1. Pharmacological: offenses that are psychopharmacology induced, that is, the result of a response to the intoxicating effects of a drug 2. The outlawing of certain drugs makes the people using these chemicals (actually, the crime is "possession" of the drugs) criminals while substantially inflating the cost of the substances for the consumer. To secure their preferred substance, those using illegal drugs typically target sources of cash or salable property and/or sell drugs. While there is a criminal population whose nondrug law violations are based only on their desire to secure drugs, an unknown percentage, perhaps a majority, were criminals whose drug use is simply part of a pattern of hedonistic and antisocial behavior. In fact, "diversion of prescription drugs for personal use by physicians is a significant problem in the United States" (Cummings, Merlo, and Cottler 2011: 195), and the addiction rate for physicians is estimated at anywhere from 30 to 100 times that for the population at large (Grosswirth 1982; Kennedy 1995; McDougal 2006). This has implications for prevention programs that focus on providing information about the dangers of drug use, discussed in Chapter 8. Eugene Boisaubin and Ruth Levine (2001: 32) note physician vulnerability: "In their early medical education [they] tend to overestimate their understanding of pharmacology and underestimate, or fail to comprehend, what addiction is and means. The relatively high rate of drug misuse among physicians can be explained by availability. Research has determined that "youngsters who have conduct problems are more likely than others to be exposed to illicit drugs" (Swan n. Adolescents with emotional and behavioral problems are more likely to abuse alcohol, tobacco, and illicit drugs. Those who were inclined toward substance abuse admitted to delinquent behaviors such as stealing, cutting classes or skipping school, and hanging around with others who get into trouble. They also report poor peer and parental relations and problems such as difficulty concentrating in school or focusing attention on tasks at home, at part-time work, or even when involved in sports. When compared to adolescents having fewer or less serious behavioral problems, those who repeatedly stole, showed physical aggression, or ran away from home were seven times as likely to be dependent on alcohol or illicit drugs. They were more than four times as likely to have used marijuana in the past month and seven times more likely to use other illicit drugs. They were nearly three times as likely to have used alcohol in the past month, three times as likely to have smoked cigarettes in the past month, and nearly nine times as likely to need treatment for drug abuse. According to the 2001 National Household Survey on Drug Abuse (discussed later), youths who engaged in violent behaviors during the past year were more likely to report past month alcohol and illicit drug use than were youths who did not engage in violent behaviors during the past year. However, "those both using and selling drugs were more than twice as likely to have started using drugs before committing crimes as were those using but not selling drugs" (Brounstein et al. In fact, we cannot be sure whether drug misuse leads to crime or criminals tend to misuse drugs (or perhaps neither); there are variables that lead to drug misuse, and the same variables lead to crime (McBride and McCoy 1981; Speckart and Anglin 1985, 1987). Indeed, areas with high levels of delinquency and crime also have high levels of drug usage, while the reverse is also true. In their study, Cheryl Carpenter and her colleagues (1988) found that the most seriously delinquent adolescents also used drugs, but crime and drug use appeared to be independent of one another, both apparently being related to other causal variables. In fact, extensive research informs us that a relatively small segment of youths commit a disproportionate amount of juvenile crime, and "the majority of serious crimes committed by youths are concentrated among serious delinquents who are also heavy users of alcohol and other drugs" (Johnson et al. For these individuals, both drug use and crime appear to be part of a troubled lifestyle. There is undoubtedly a high correlation between drug use and nondrug crime (Gandossy et al. The question of whether crime is a predrug use or postdrug use phenomenon is actually an oversimplification, and James Inciardi (1981: 59) argues, "the pursuit of some simple cause-and-effect relationship may be futile. In the population of female heroin users criminal activity occurred after both alcohol and other drug abuse and marijuana use but before involvement with the more debilitating barbiturates and heroin. If drug users simply continue in crime after they have given up drugs, efforts to reduce crime by reducing drug use are doomed to fail. Wilson (1975: 137) points out, perhaps "some addicts who steal to support their habit come to regard crime as more profitable than normal employment. They would probably continue to steal to provide themselves with an income even after they no longer needed to use part of that income to buy heroin" or any other illegal substance. For example, James Vorenberg and Irving Lukoff (1973) found that the criminal careers of a substantial segment of the heroin addicts they studied antedated the onset of heroin use. Furthermore, they found that those whose criminality preceded heroin use tended to be more involved in violent criminal behavior.
Buy 100mcg rhinocort amex
Diabetes-specific enteral nutrition formula in hyperglycemic allergy testing johannesburg rhinocort 100mcg line, mechanically ventilated allergy shots types cheap rhinocort amex, critically ill patients: a prospective, open-label, blind-randomized, multicenter study. Insulin therapy and glycemic control in hospitalized patients with diabetes during enteral nutrition therapy: a randomized controlled clinical trial. Use of insulin glargine in patients with hyperglycaemia receiving artificial nutrition. Comparison of 70/30 biphasic insulin with glargine/lispro regimen in non-critically ill diabetic patients on continuous enteral nutrition therapy. A practical and evidence-based approach to management of inpatient diabetes in non-critically ill patients and special clinical populations. Effect of low-calorie parenteral nutrition on the incidence and severity of hyperglycemia in surgical patients: a randomized, controlled trial. A double-blind, randomized clinical trial comparing soybean oil-based versus olive oil-based lipid emulsions in adult medical-surgical intensive care unit patients requiring parenteral nutrition. Evaluation of nonglucose carbohydrates in parenteral nutrition for diabetic patients. Glargine insulin use versus continuous regular insulin in diabetic surgical noncritically ill patients receiving parenteral nutrition: randomized controlled study. Common reasons include decreased insulin clearance, reduced elimination of non-insulin glucoselowering therapies, reduced renal gluconeogenesis, gastroparesis, increased glycemic variability, hypoglycemic unawareness, improved insulin sensitivity following initiation of renal replacement therapy, and decreased food intake due to poor appetite or lack of timely access to food. Knowledge about which non-insulin glucose-lowering agent(s) can be used effectively and safely for this population in the inpatient setting is important. Management includes specific treatments according to underlying cause and supportive treatment to prevent and manage complications. In addition, other patients may develop transient hyperglycemia detected during admission that normalizes after discharge, so-called "stress hyperglycemia". In patients with renal insufficiency, decreased renal gluconeogenesis, lack of gluconeogenic substrates with decreased food intake or lack of timely access to food, increased glycemic variability, decreased renal degradation and excretion of insulin, decreased elimination of other glucose-lowering therapies, improved insulin sensitivity following initiation of renal replacement therapy, and impairment of counter-regulatory hormonal responses, can all lead to hypoglycemia (2,9). In the early years after diagnosis of diabetes, therapy is aimed at "normalizing" glycemic control (while minimizing the risk of hypoglycemia) and inducing metabolic memory in order to decrease the risk of long-term microvascular (including diabetic kidney disease) and macrovascular complications (12,13). The aims of insulin therapy in diabetes patients on maintenance hemodialysis are to improve the quality of life and avoid the extremes of hypoand hyperglycemia. Inherent risks, including severe hypoglycemia and increased cardiovascular risk, should be considered when formulating therapeutic strategies in this setting (12,13). In addition, knowledge about which non-insulin glucose-lowering agent(s) can be used safely and effectively for this population in-hospital is also important (2,8,10). Approximately 57% of 2,040,206 glucose measurements collected in this database were from patients during hospitalization. Optimizing individualized glycemic control requires an understanding of the altered pharmacokinetics and pharmacodynamics of insulin as well as many other factors in this setting. Since endogenous insulin is secreted via the portal vein, the liver metabolizes 50% of insulin in the first pass. The kidney plays a secondary role in the metabolism of endogenous insulin but will clear 65% of insulin reaching it. In contrast, exogenous insulin is absorbed systemically, and thus the kidney plays a primary role in the metabolism of injected therapeutic insulin (19). For example, around 65% of dialysis patients have HbA1C <7% (53 mmol/mol), and 35% HbA1C <6% (42 mmol/mol). These levels have no prognostic benefit in this population and an appropriate review of insulin and/or non-insulin therapies and glycemic targets should be undertaken. A study using the euglycemic clamp technique demonstrated a 25% reduction in basal insulin requirements on the day after dialysis as compared with the day before dialysis, with no difference in mealtime insulin needs (25). Mean HbA1C on admission was 8% (64 mmol/mol); and 76% of patients were treated with insulin prior to admission. Although the glucose-lowering effect of the different insulin doses was no different, there was a 50% reduction in the frequency of hypoglycemia in the lower dose group. Some glucose-lowering medications also have beneficial effects on the kidney that are direct. The continual use of these drugs or alternatives should be reviewed as part of ongoing care and discharge planning.
Order rhinocort
Under these circumstances allergy medicine zyrtec vs claritin order rhinocort without a prescription, emergent thyroidectomy may represent the most effective and rapid way of resolving thyrotoxicosis allergy symptoms vs cold symptoms order rhinocort with a mastercard. Introduction Amiodarone is a benzofuranic iodine-rich drug structurally similar to thyroid hormones (1,2). Pathophysiology Abnormal thyroid function tests, not indicative of thyroid dysfunction, are found in all patients who have been given amiodarone. Thus, in addition to changes in serum thyroid hormones concentrations, a "hypothyroid-like effect" in peripheral tissue may also occur. Amiodarone-induced thyroid dysfunction may result from excessive iodine load and/or the intrinsic properties of the drug (1,6). After iodine load, the thyroid gland normally blocks thyroid hormone synthesis (the Wolff-Chaikoff effect). Histopathological changes look like those seen in other thyroid-destructive processes, such as subacute thyroiditis. Amiodarone-Induced Thyroid Disease the overall prevalence of amiodaroneinduced thyroid dysfunction, though widely Amiodarone-Induced Thyrotoxicosis variable in different series, is between 15% and 20%, but may increase to 36% or 49% in patients with congenital heart disease, -thalassemia major or under phenytoin therapy (1). Amiodarone therapy is not associated with de novo development of thyroid autoimmunity. In iodine-replete areas the higher sensitivity of the thyroid gland to generate an iodine-induced turnoff signal for hormone biosynthesis makes it relatively resistant to the iodine load. This may imply that a high intrathyroidal drug concentration needs to be reached before the damage of thyroid follicular cell becomes evident at a clinical level. Fausto Bogazzi, Luca Tomisti, Luigi Bartalena, and Enio Martino "mixed" forms might be found in a subset of patients with an underlying multinodular goiter. Likewise, iodine-induced hyperthyroidism is unlikely to play a pathogenic role in patients with a normal thyroid gland. Additional radioisotopic techniques using a different tracer still need to be validated (13). However, conventional echography does not provide functional information, and the presence of goiter or nodules does not necessarily imply that an increased thyroid hormone synthesis is the underlying pathogenic mechanism. On the other hand, the role of the cardiologist is: r to evaluate the underlying cardiac disease; r to evaluate the equilibrium of cardiac funcr to estimate the risk of an impending worsening of cardiologic conditions. This is obviously not an ideal situation in patients with underlying cardiac problems, whose hyperthyroidism should be promptly controlled. To increase the sensitivity of the thyroid gland and the response to thionamides, sodium perchlorate, which decreases thyroid iodine uptake, has been used. Thionamide therapy can be continued until euthyroidism is restored, if this is permitted by the underlying heart disease and cardiocirculatory compensation. After restoration of euthyroidism, definitive therapy of the hyperfunctioning thyroid gland should be considered. If amiodarone can be discontinued, radioiodine therapy can be performed after iodine contamination is over, as suggested by normalized iodine urinary excretion. The risk may be reduced if patients are treated preventively with a course of thionamides (17). This is usually required, although mild forms may be transient and self-limiting, requiring only watchful waiting, if this is compatible with the underlying cardiac conditions. If amiodarone can be discontinued, restoration of euthyroidism is achieved with a median time of about 30 days. If amiodarone therapy must be continued, glucocorticoids may be started, and euthyroidism can be induced even continuing amiodarone (20), although there may be a higher risk of thyrotoxicosis recurrence during treatment (21). Discontinuation of amiodarone therapy is advisable, if feasible, to reduce the recurrence rate of thyrotoxicosis, to allow a prompt and stable restoration of euthyroidism, and to shorten the exposure of the heart to thyroid hormone excess (21). After restoration of euthyroidism, periodical assessment of thyroid status is required, because >15% of patients will develop permanent hypothyroidism over time, requiring levothyroxine replacement therapy (22). However, owing to very limited experience in this subset of patients and to the risk of exacerbation of Fausto Bogazzi, Luca Tomisti, Luigi Bartalena, and Enio Martino Proportion of patients remaining thyrotoxic 1.
Generic 100mcg rhinocort fast delivery
The catheter is gently agitated up and down as the suture line moves around the orifice to ensure that it is not compromised by generous suture stitches as they pass outside of the aorta allergy medicine behind the counter buy cheap rhinocort 200mcg. If reconstruction is desired allergy treatment in homeopathy generic rhinocort 200mcg on line, it can usually be accomplished through an inclusion button anastomosis. Intercostal arteries in the region of a proximal or distal aortic anastomosis can be reconstructed using a long, beveled suture line. Distal anastomosis the author makes every effort to perform tube reconstructions to the aortic bifurcation unless there is gross aneurysmal disease of the common iliac arteries. Results of treatment and complications 227 Extending the reconstruction to the iliac or femoral arteries is only performed when no other technical alternative exists. Indeed, careful attention to hemostasis from the beginning of the operation, combined with minimal heparin use, is an important component of care. Careful inspection of the inferior aspect of the entire aneurysm sac is necessary to detect back-bleeding lumbar/intercostal vessels that can be a source of significant postoperative hemorrhage. The redundant aneurysm sac is sutured over the aortic prosthesis in the abdomen and chest. As the left kidney is returned to its anatomic position, the perinephric fat usually suffices to provide adequate coverage of the aortic graft in the region of the visceral aortic segment. A single pleural tube is placed and a closed suction drain may be left in the retroperitoneum if hemostasis is in question. Renal failure Minimizing renal ischemic times, using cold perfusate, avoiding intraoperative hypotension, and treating stenotic lesions aggressively with either bypass or open stent placement reduce renal injury. The author reserves dialysis for specific clinical indications like volume overload, hyperkalemia, or acidosis. When needed, continuous venovenous hemodialysis is preferred because it provides for a smoother hemodynamic course than conventional hemodialysis. Preoperative renal insufficiency is the most powerful predictor of postoperative renal failure; postoperative renal dysfunction negatively affects short- and long-term survival. Indeed, if strict criteria are used, some 40% of patients suffer a respiratory complication. Contributing factors include paralysis of the left hemidiaphragm and pain from the extensive chest wall incision that impedes pulmonary hygiene. For patients who fail extubation, the author favors early placement of a tracheostomy (required in <10% of patients). Postoperative care Postoperatively, patients should be monitored in an intensive care unit setting. Oxygen delivery is important in the early phase of recovery and the author rarely extubates patients in the early postoperative period. It is important to monitor the hematocrit for signs of ongoing bleeding and all coagulation disorders should be aggressively corrected. Most late aortic events are the result of native aneurysmal disease in remote (or noncontiguous) aortic segments. Several reports have emerged validating that most operative survivors return to their preoperative independent living status. Contemporary management of descending thoracic and thoracoabdominal aortic aneurysms: endovascular versus open. In addition, late aortic events occur in about 10% of patients, but few of these are graft-related. These features increase the incidence of injury to both vascular and visceral retroperitoneal structures during aneurysm repair. As a result, the special considerations in the open reconstruction for inflammatory aortic aneurysms are still worthy of study and review for both vascular surgeons and trainees. The likelihood of these technical difficulties increases as the extent of the aneurysm and size of the inflammatory mass increase. Inflammatory aortic aneurysms occur at a younger age, have a stronger familial tendency, and occur more predominantly in men compared to noninflammatory aneurysms. The majority are symptomatic at presentation with abdominal or back pain, weight loss, and elevated erythrocyte sedimentation rate as common clinical findings.
References: