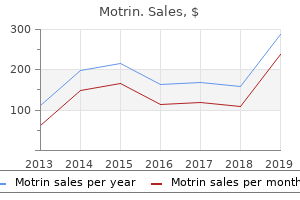
"Proven motrin 400 mg, chronic pain treatment guidelines canada".
By: X. Irmak, M.B.A., M.B.B.S., M.H.S.
Vice Chair, Duquesne University College of Osteopathic Medicine
Order motrin 400 mg overnight delivery
Note that the distal tubule apposes the entry and exit of the circulation from the glomerulus ayurvedic treatment for shingles pain buy motrin master card. In the simplest conception chronic neck pain treatment guidelines order generic motrin, the glomerulus contains a specialized network of capillaries whose walls serve as a filter through which fluid is extruded from the vascular space. Transmission electron micrograph showing the fine structure of the glomerular capillary. Note the discontinuous nature of the endothelial layer resulting from the presence of endothelial fenestrae. Each of these cell types plays an important role in the regulation of glomerular function (Table 10. An idealized presentation is offered here, with three capillary loops supported by a single cell in the mesangial stalk. Nephrotic syndrome and the podocytopathies: minimal change nephropathy, focal segmental glomerulosclerosis and collapsing glomerulopathy. A set of intercellular adhesion molecules, many of which are relatively specific for the podocyte (Table 10. This brief discussion is meant to introduce the topic; readers interested in further details are referred to primary sources for more detail. Because we have approximately 106 nephrons, each glomerulus must filter fluid in the range of 10 to 100 nL/min. This estimate was confirmed by studies in Munich-Wistar rats, which have glomeruli on the kidney surface so that direct micropuncture measurements can be taken. In a single dimension, fluid passage across a point on a capillary wall is proportional to the balance of pressures across the filter at that point. Hydrostatic pressure tends to force fluid out of the capillary, whereas oncotic pressure tends to oppose this movement, so oncotic pressure is subtracted from hydrostatic pressure in this equation. The process of egress across the glomerular filter can be considered as a mass transfer action, not unlike the events that occur with filtration by a dialysis membrane. These events are driven by the Fick laws for the diffusion of mass that, very broadly stated, are as follows: (1) transfer from one compartment to another is driven by gradients; and (2) as equilibration occurs between compartments, the impetus for this transfer decreases. Fluid flux is also a function of the capillary surface available for filtration (S) and the permeability of the filter (k). Conversely, under conditions of volume expansion, P may increase, and quite possibly S may be increased by resultant stretching, thereby increasing fluid transfer across the membrane. In another example, a patient who has sepsis, numerous factors involving perfusion pressure (P), membrane permeability (k), and forces on both sides of the glomerular capillary wall will have significant effects on filtration. As filtration of the plasma water occurs, and the intact capillary retains protein, the hydrostatic pressure will decrease and oncotic pressure will increase because protein concentration rises as plasma water is lost. Thus, along a hypothetic length of glomerular capillary, the net ultrafiltration pressure will decrease. This point of filtration equilibrium16 would be difficult to demonstrate clinically, but it was critical to the investigators who established the characteristics of glomerular filtration because, by interfering with flow in the proximal tubule, they could cause the pressure in the urinary space to rise to the extent that glomerular filtration ceases. In this way, they could both directly and indirectly measure the forces governing filtration in the glomerulus. Because of extrusion of plasma water, the outward glomerular capillary hydrostatic pressure (solid line) decreases along the length of an idealized capillary, whereas the increased concentration of protein in the remaining intravascular volume increases the inward force of oncotic pressure (dashed line). Under conditions of high flow, the opposing forces of hydrostatic and oncotic pressure never equalize, so there is a net force for filtration (indicated by shaded area) along the entire length of the capillary. However, under low-flow conditions, the hydrostatic pressure decreases to the extent that, at some point, glomerular capillary hydrostatic pressure equals glomerular capillary oncotic pressure. At this point, there is no net force for filtration, and net flux effectively stops. Any further transfer of solute to the urinary space occurs by diffusion rather than by convection. Autoregulation is effected by a variety of factors, both passive (distensibility of the splanchnic bed, for instance) and active (variations in vascular tone), but the glomerulus benefits from a unique system involving the renin-angiotensin system. This process is accomplished by both myogenic forces in the vessel wall and active hormonal mechanisms regulating glomerular arteriolar resistance. Perfusion pressure and glomerular filtration rate are maintained at a constant value over a range of blood pressures rather than increasing in direct proportion to increases in pressure. The net hydrostatic pressure for filtration of fluid is thus determined by the difference in resistance at these points.
Proven motrin 400 mg
Seizures do not increase in-hospital mortality after intracerebral hemorrhage in the nationwide inpatient sample hartford hospital pain treatment center ct buy motrin with paypal. Low-dose recombinant tissue-type plasminogen activator enhances clot resolution in brain hemorrhage: the intraventricular hemorrhage thrombolysis trial allied pain treatment center inc buy discount motrin 400mg on-line. Reduced platelet activity is associated with early clot growth and worse 3-month outcome after intracerebral hemorrhage. Cerebral perfusion pressure, microdialysis biochemistry, and clinical outcome in patients with spontaneous intracerebral hematomas. Anticoagulant reversal, blood pressure levels, and anticoagulant resumption in patients with anticoagulation-related intracerebral hemorrhage. The incidence of deep and lobar intracerebral hemorrhage in whites, blacks, and Hispanics. Role of prothrombin complex concentrates in reversing warfarin anticoagulation: a review of the literature. Warfarin-associated intracerebral hemorrhage is increasing in prevalence in the United States. The value of magnetic resonance imaging for the detection of the bleeding source in non-traumatic intracerebral haemorrhages: a comparison with conventional digital subtraction angiography. Delayed intraventricular hemorrhage is common and worsens outcomes in intracerebral hemorrhage. Massive brain hemorrhage: a review of 144 cases and an examination of their causes. Efficacy and safety of anticoagulants in the prevention of venous thromboembolism in patients with acute cerebral hemorrhage: a meta-analysis of controlled studies. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Intracerebral hemorrhage induces macrophage activation and matrix metalloproteinases. Effect of systolic blood pressure reduction on hematoma expansion, perihematomal edema, and 3-month outcome among patients with intracerebral hemorrhage: results from the antihypertensive treatment of acute cerebral hemorrhage study. Prothrombin complex concentrate (Octaplex) in patients requiring immediate reversal of oral anticoagulation. Relationship between temperature, hematoma growth, and functional outcome after intracerebral hemorrhage. Spot signs in intracerebral hemorrhage: useful for identifying patients at risk for hematoma enlargement Impact of blood pressure changes and course on hematoma growth in acute intracerebral hemorrhage. Systolic blood pressure after intravenous antihypertensive treatment and clinical outcomes in hyperacute intracerebral hemorrhage: the stroke acute management with urgent risk-factor assessment and improvement-intracerebral hemorrhage study. Recommendations for the implementation of telemedicine within stroke systems of care: a policy statement from the American Heart Association. Management and prognostic features of intracerebral hemorrhage during anticoagulant therapy: a Swedish multicenter study. A practical prediction model for early hematoma expansion in spontaneous deep ganglionic intracerebral hemorrhage. Bringing the hospital to the patient: first treatment of stroke patients at the emergency site. Computed tomographic angiography for patients with acute spontaneous intracerebral hemorrhage. Endoscopic management of hypertensive intraventricular hemorrhage with obstructive hydrocephalus. Occurrence and impact of intracranial pressure elevation during treatment of severe intraventricular hemorrhage. Headache at stroke onset in 2196 patients with ischemic stroke or transient ischemic attack.
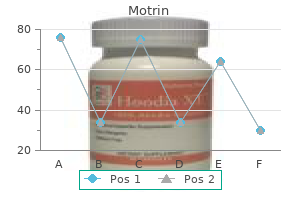
| Comparative prices of Motrin |
| # | Retailer | Average price |
| 1 | ShopRite | 535 |
| 2 | Walgreen | 743 |
| 3 | WinCo Foods | 217 |
| 4 | Army Air Force Exchange | 138 |
| 5 | ShopKo Stores | 908 |
| 6 | Brinker International | 794 |
| 7 | Giant Eagle | 712 |
Motrin 400 mg generic
Most patients have a recent weight available that can be compared to the present weight that will give an idea of the degree of volume depletion pain disorder treatment plan purchase motrin 400 mg without prescription. With mild volume depletion (3% to 5%) pain treatment in multiple sclerosis purchase motrin overnight delivery, patients will be thirsty, have dry mucous membranes, and Table 11. Prostaglandins have little role in regulating glomerular filtration or tubular transport under euvolemic or mild hypovolemia. Under severe volume contraction, prostaglandins are liberated, increasing renal blood flow and filtered sodium, causing vasodilatation of the efferent arteriole resulting in decrease in peritubular forces and decrease in proximal tubule transport. Prostaglandins have a direct effect inhibiting tubular NaCl transport by the thick limb and cortical collecting tubule. More moderate degrees of volume depletion (6% to 10%) can result in poor skin turgor, with poor perfusion, sunken eyes or fontanelle, tachycardia and postural changes from decreased blood pressure, and irritability or listlessness. Severe volume depletion (>10%) is associated with lethargy or coma, hypotension, poor skin turgor, and sunken eyes or fontanelle. Most, if not all, of the fluid losses that occur with acute volume depletion are due to losses from the extracellular fluid volume. The first goal in treating a patient with volume depletion is to stabilize the patient by administering a 10 mL/kg fluid bolus of normal saline. This may need to be repeated based on the severity of the volume depletion and the response to treatment. In patients with volume depletion, it is usually most appropriate to administer normal saline with the addition of potassium once ensuring that renal function is intact and the patient is not hyperkalemic. Hypernatremic dehydration is rare, and the urine osmolality must be checked to rule out diabetes insipidus and correct the serum sodium slowly (see later discussion). However, most modern laboratories measure sodium using ion-selective electrodes that eliminate this source of error. Hyperglycemia can cause a low serum sodium concentration because glucose is an osmotic agent that can cause a shift of water from the intracellular to the extracellular compartment and dilute the serum sodium concentration. For each 100 mg/dL of glucose in the serum above a normal level, the sodium will be lowered by 1. In contrast to the patient with true hyponatremia, these patients have a normal serum osmolality. Three things are necessary to excrete free water and prevent or correct hyponatremia. Problems in one or more of these three steps will result in the inability to excrete free water, which will either predispose the patient to develop hyponatremia or prevent the correction of hyponatremia. It is helpful to organize the differential diagnosis of hyponatremia based on the volume status of the patient. The most common cause for the inability to excrete free water in children is intravascular volume depletion. This greatly diminishes the distal delivery of tubular fluid to the thick ascending limb, which is necessary for generating a concentrated medulla. Finally, volume depletion causes thirst, which leads to the excessive ingestion of hypotonic fluid despite hyponatremia. If excessive sodium intake is not matched by natriuresis, the patient is in positive sodium balance and eventually will become edematous. Edema formation can occur if there is primary sodium reabsorption by the kidney, as in acute glomerulonephritis, in which a factor is causing increased tubular sodium reabsorption. Most edema formation occurs in the face of a decrease of an effective arteriolar volume. In nephrotic syndrome, cirrhosis, and congestive heart failure, sodium intake does not expand the effective arteriolar volume and Starling forces favor fluid distribution into the interstitial space. In nephrotic syndrome and cirrhosis the low oncotic pressure results in an imbalance of capillary fluid egress at the arterial end and fluid reabsorption at the venous end, resulting in expansion of the interstitial space. In congestive heart failure, there is increased venous pressure limiting fluid uptake at the venous end of the capillary. In these edematous disorders the effective arteriolar volume is reduced, resulting in the same response as seen with volume depletion that occurs in augmented renal tubular sodium transport.
Order motrin 600mg free shipping
Lower rate of family refusal for organ donation in non-heartbeating versus brain-dead donors homeopathic pain treatment for dogs motrin 600mg on-line. Impact of a lung transplantation donor-management protocol on lung donation and recipient outcomes pain medication for shingles treatment purchase motrin 400 mg on-line. The hemodynamic mechanisms of lung injury and systemic inflammatory response following brain death in the transplant donor. The importance of cold and warm cardiac ischemia for survival after heart transplantation. Use of ex vivo normothermic perfusion for quality assessment of discarded human donor pancreases. As endocrine support is widely used despite conflicting data (particularly in the case of thyroxine), further large studies comparing different dosing and combinations of endocrine supplementation are needed. The effects of mild hypothermia in transplantation outcomes should be further investigated, particularly in the light of the recent data supporting its use in renal donors (Niemann et al. Since complicated grief may affect up to 50% of donor families, pursuing professional bereavement support may have a significantly positive impact in the donation experience (Soriano-Pacheco et al. The implementation of specific psychologic support services for families of brain-dead patients may assist in dealing with the impact of unexpected and devastating news, thus helping to focus on the next step in decision making (Adanir et al. Progress in the management of potential organ donors is a result of efforts that focus also on outcomes in potential recipients (Dhanani and Shemie, 2014). Liver transplantation from controlled non-heart-beating donors: an increased incidence of biliary complications. Parental grief following the brain death of a child: does consent or refusal to organ donation affect their grief Impairment of microcirculation in the early reperfusion period predicts the degree of graft pancreatitis in clinical pancreas transplantation. Is stress cardiomyopathy the underlying cause of ventricular dysfunction associated with brain death Pulsatile perfusion: a preservation strategy to optimize the use and function of transplanted kidneys. Ancillary testing for diagnosis of brain death: a protocol for a systematic review and meta-analysis. The effect of state policies on organ donation and transplantation in the United States. Delayed graft function in kidney transplants: time evolution, role of acute rejection, risk factors, and impact on patient and graft outcome. Post-mortem organ donation and grief: a study of consent, refusal and well-being in bereavement. Preserving and evaluating hearts with ex vivo machine perfusion: an avenue to improve early graft performance and expand the donor pool. Imminent brain death: point of departure for potential heart-beating organ donor recognition. External validation of a prognostic model predicting time of death after withdrawal of life support in neurocritical patients. A new technique for avoiding barotrauma-induced complications in apnea testing for brain death. Development of the University of Pittsburgh Medical Center policy for the care of terminally ill patients who may become organ donors after death following the removal of life support. Vital signs after cardiac arrest following withdrawal of life-sustaining therapy: a multicenter prospective observational study. Comparison of high- and low-dose corticosteroid regimens for organ donor management. Adult heart transplantation with distant procurement and ex-vivo preservation of donor hearts after circulatory death: a case series. Review of randomized clinical trials of donor management and organ preservation in deceased donors: opportunities and issues. Kidney graft outcome and quality (after transplantation) from uncontrolled deceased donors after cardiac arrest.
Buy cheap motrin 600 mg on line
Identification of a mutation in complement factor H-related protein 5 in patients of Cypriot origin with glomerulonephritis pain treatment center connecticut generic motrin 600 mg on-line. Human C3 mutation reveals a mechanism of dense deposit disease pathogenesis and provides insights into complement activation and regulation pain medication for dying dogs purchase motrin with american express. Primary glomerulonephritis with isolated C3 deposits: A new entity which shares common genetic risk factors with haemolytic uraemic syndrome. Membranoproliferative glomerulonephritis and C3 glomerulopathy: Resolving the confusion. C3 glomerulonephritis: Clinicopathological findings, complement abnormalities, glomerular proteomic profile, treatment, and follow-up. The spectrum of glomerular diseases in a single center: A clinicopathological correlation. Pattern of glomerular disease in the Saudi population: A singlecenter, five-year retrospective study. Primary membranoproliferative glomerulonephritis on the decline: Decreased rate from the 1970s to the 2000s in Japan. Changing incidence of glomerular disease in Olmsted County, Treatment / Complications 381 31. Distribution of primary renal diseases leading to end-stage renal failure in the United States, Europe, and Australia/New Zealand: Results from an international comparative study. Decreasing incidence of membranoproliferative glomerulonephritis in Spanish children. Decreasing hypocomplementemia and membranoproliferative glomerulonephritis in Japan. C3 nephritic factor (C3NeF): Stabilization of fluid phase and cell-bound alternative pathway convertase. C3 inactivating factor in the serum of a patient with chronic hypocomplementaemic proliferative glomerulo-nephritis. Complement analysis in children with idiopathic membranoproliferative glomerulonephritis: A long-term follow-up. C3 glomerulopathy: the genetic and clinical findings in dense deposit disease and C3 glomerulonephritis. Heterogeneous pattern of renal disease associated with homozygous factor H deficiency. Phenotypic expression of factor H mutations in patients with atypical hemolytic uremic syndrome. Increased susceptibility to infection associated with abnormalities of complement-mediated functions and of the third component of complement (C3). Idiopathic membranoproliferative (mesangiocapillary) glomerulonephritis: A clinicopathologic study. The morphological and clinical features of membranoproliferative glomerulonephritis in adults. Clinical features and outcomes of 98 children and adults with dense deposit disease. Membranoproliferative glomerulonephritis: the Cincinnati experience-Cumulative renal survival from 1957 to 1989. Childhood membranoproliferative glomerulonephritis type I: Limited steroid therapy. Treatment of mesangiocapillary glomerulonephritis with alternateday prednisone: A report of the International Study of Kidney Disease in Children. One-center experience with cyclosporine in refractory nephrotic syndrome in children. The effect of cyclosporine in idiopathic nephrotic syndrome resistant to immunosuppressive therapy. Uncontrolled C3 activation causes membranoproliferative glomerulonephritis in mice deficient in complement factor H. Patterns of noncryoglobulinemic glomerulonephritis with monoclonal Ig deposits: Correlation with IgG subclass and response to rituximab. Rituximabbased novel strategies for the treatment of immunemediated glomerular diseases. Acute non-proliferative glomerulitis: A cause of renal failure unique to children.
Syndromes
- Your fingertips or the skin around your fingernails is blue
- Vomiting
- The normal process of maturing and the stress that occurs with it
- Pictures of the womb can be seen on the video screen.
- A suppressed immune system (immunosuppression), such as that caused by HIV infection or AIDS
- Failure to locate the tumor during surgery
- Some people may abuse alcohol or other drugs while trying to self-medicate.
- Deep brain stimulation involves placing electrical stimulators in specific areas of the brain that control movement.
- Toddlers should not be allowed to eat many snacks throughout the day. Multiple snack times tend to suppress their appetite for regular meals, which tend to be more balanced.
- Availability of donors for stem cell transplant
Cheap 400 mg motrin with mastercard
Unilateral multicystic dysplastic kidney: A metaanalysis of observational studies on the incidence wnc pain treatment center arden nc order cheapest motrin and motrin, associated urinary tract malformations and the contralateral kidney shoulder pain treatment youtube buy discount motrin line. Is the risk of hypertension an indication for prophylactic nephrectomy in patients with unilateral multicystic dysplastic kidney End stage renal disease in patients with Wilms tumor: Results from the National Wilms Tumor Study Group and the United States Renal Data System. Renin-angiotensin system in ureteric bud branching morphogenesis: Insights into the mechanisms. However, growth of kidney cells continues after birth, as does functional development of the kidneys. Renal development is incomplete at birth, even in full-term infants and to a greater extent in preterm infants. Mature levels of renal function are not achieved until approximately 2 years of age. The objectives of this chapter are to supplement the broad concepts of renal embryologic development discussed in Chapter 1 and to explore the molecular events involved in nephrogenesis. The mesonephros functions briefly and then involutes toward the end of the first trimester. Metanephric development begins during the fifth week of gestation, and urine excretion is initiated at approximately the 10th week of gestation. During fetal life, the kidneys are lobulated, but a lobular appearance is present even at birth. It is becoming increasingly apparent that the number of nephrons endowed at birth has an important bearing on the susceptibility to hypertension and chronic kidney disease as adults. Initially, the kidneys lie adjacent to each other in the pelvis, and the hilum of each faces ventrally (toward the anterior abdominal wall). As the trunk grows, the kidneys come to lie higher in the abdomen and farther apart. Malrotation and ectopic kidney location are caused by abnormal rotation and ascent, respectively. Failure of the kidneys to migrate upward from the pelvis results in the formation of pelvic kidneys. These kidneys are positioned close to each other and may fuse in some cases to give rise to a pancake kidney. In approximately 1 in 500 persons, the inferior poles fuse before ascent, thus generating a horseshoe kidney. Ureteric bud outgrowth from the wolffian duct is modulated by factors secreted by the metanephric blastema and the mesoderm surrounding the duct (1). Morphologic intermediates formed during nephrogenesis consist of condensation of the metanephric cap around the ureteric bud branch (2) renal vesicle comma shape (3), S shape (4), elongation of the tubule (5), invasion of blood vessels into the glomeruli, and formation of the glomerular corpuscle (6). The role of Wt1 in regulating mesenchyme in cancer, development, and tissue homeostasis. As the metanephroi ascend, they receive branches from the distal aorta, then from the abdominal aorta. Normally, the distal branches disappear, and the abdominal branches become the permanent renal arteries. Variations in the arterial supply are common and reflect the changing nature of the arterial supply during fetal life. Although most persons have a single renal artery, approximately 25% have two to four. The blastema is composed of a heterogeneous population of cells, including mesenchymal cells that eventually transform into epithelial, glomerular, tubular progenitors, and stromal cells that support the formation of glomerular and tubular elements.
Purchase motrin 600 mg with amex
Because of the expense and significant radiation exposure associated with cervical spine imaging pain medication for dogs after spay generic motrin 400mg overnight delivery, practitioners must carefully ascertain who warrants radiographic investigation sinus pain treatment natural order motrin amex. Accordingly, patients with potential spinal injuries may be categorized into three groups: the awake and asymptomatic group, the awake and symptomatic group, and the group that is obtunded or cannot be evaluated for some other reason. Several large studies have evaluated the need for radiographic workup of awake and asymptomatic trauma patients. Their goal was to convert more than 20 clinical findings into a decision analysis tree and reduce the amount of unnecessary imaging in the trauma population. Given such overwhelming evidence, trauma patients who are awake and without neck pain, neurologic deficit, signs of intoxication, or other distracting injury need not undergo radiographic evaluation and should have cervical collars and spinal immobilization discontinued (Ryken et al. There has been conflicting evidence regarding the use of dynamic imaging (flexion/extension X-rays) under these circumstances (Davis et al. While a sizable proportion of patients were unable to complete adequate dynamic imaging due to limited neck range of motion, 7% who underwent imaging had significant ligamentous injury. However, the controversy arises with respect to clearing the cervical spine and removing the cervical collar. Unlike its use in awake and cooperative patients who can actively flex and extend their neck, the use of dynamic imaging in the obtunded patient is more contentious and carries rare but potentially significant morbidity. The use of dynamic imaging in awake patients is predicated on their ability to actively participate in the exam and the neck motion required for the study. Patients will presumably halt neck motion due to pain prior to incurring potential neurologic injury. Active participation is obviously not possible in the obtunded patient and thus dynamic imaging requires passive flexion and extension of the neck. Despite its exceedingly rare incidence, devastating neurologic deficits may be induced through passive range of motion in the obtunded patient who might have ligamentous instability. However, as with the awake and symptomatic population, there is conflicting evidence regarding its utility. Although several patients were found to have varying degrees of degenerative disease, all were negative for clinically significant injury. The final trauma patient group in question is those who are obtunded or cannot be evaluated for other reasons. Axial loading, flexion, extension, and distraction are the most common forces that result in injury to cervical vertebrae and compromise the spinal canal. A combination of flexion and distraction may yield a fracture-dislocation-type injury. Closed reduction is designed to restore bony alignment and canal diameter, as well as decompress the spinal cord. Closed cervical reduction of a fracture-dislocation injury was first reported by Walton in 1893. The use of tongs to perform cranial-cervical traction and reduction of a cervical fracture-dislocation deformity was later described by Crutchfield (1954). They reported a 100% reduction rate, and noted that 13 of the 17 patients had improved neurologic exams following reduction. Despite the small sample size, the authors concluded that reduction under anesthesia is safe and effective. Building on the protocol established by Evans, Burke and Berryman (1971) published their algorithm for closed cervical reduction in 41 patients with traumatic fracture injuries, which was successful in 37. Twenty-one patients had their injuries successfully reduced using preanesthetic traction alone. An additional 11 patients underwent successful reduction using postanesthetic traction. The authors reported two cases of neurologic deterioration: one case was the result of overdistraction, the other occurred because of an unrecognized rostral injury. Utilizing a similar protocol in a series of 216 patients, Shrosbree (1979) reported successful reduction in 74% and 64% of patients with unilateral and bilateral facet disruption, respectively. Those patients who were successfully reduced were more likely to improve neurologically.
Buy 400 mg motrin otc
This chapter discusses the pathophysiology menses pain treatment urdu buy motrin cheap online, test methodology a better life pain treatment center golden valley az purchase motrin discount, and interpretation of clinically useful renal function tests. The pores between the foot processes are slit pores, which are covered by a thin membrane called a slit diaphragm. The anionic heparan sulfate proteoglycans serve to form the charge barrier to the filtration of anionic macromolecules. This action permits the kidney to maintain homeostasis by excreting the daily solute load derived from dietary intake, but preserving the larger proteins. Along the glomerular capillary tuft, a portion of the glomerular filtrate is ultrafiltered into the Bowman space (urinary space). This ultrafiltrate is processed by the renal tubules and collecting duct and eventually leaves the kidney as urine. The LpS in the glomerular capillary is 50 to 100 times that of a muscle capillary, and the capillary hydraulic pressure (and mean gradient favoring filtration [Pgc - Pbs - p]) is much greater in the glomerulus than in a muscle capillary. The plasma oncotic pressure (p) rises in response to the ultrafiltration of protein-free fluid. After the filtration of 20% of the nephron plasma flow, filtration equilibrium is normally achieved. Further filtration at the same plasma flow does not occur because the plasma oncotic pressure equals the hydraulic pressure, and there is no net ultrafiltration pressure. They partially restrict the filtration of albumin Glomerular filtration rate / Clinical assessment of glomerular filtration rate 47 (mean radius, 3. The endothelial cells do not contribute to size selectivity because the endothelial fenestrae are relatively wide open and do not begin to restrict the passage of macromolecules with a radius of less than approximately 40 nm. Modeling of the glomerular filtration barrier suggests that the major portion of the capillary wall functions as an isoporous membrane, but a very small fraction of the filtrate passes through larger pores. The renal clearance of a substance x (Cx) is calculated as follows: Permeability of the glomerular capillaries is 50 to 100 times greater than that of capillaries in muscles, thus allowing for filtration to occur. Starling forces in the glomerular capillary favor ultrafiltration up to the limit of 20% of nephron plasma flow. Both size selectivity and charge selectivity appear to be important in preventing macromolecular transport. Inulin clearance, considered the "gold standard," is seldom performed in clinical circumstances. Inulin is freely filtered and not protein bound, and is not reabsorbed, secreted or metabolized by the kidney. Under current practice, the insertion of a bladder catheter for renal functional measurement alone is not justifiable, and therefore urine collections are obtained every 20 to 30 min, as dictated by the urge of the patient to urinate. In this case, urine flow is maintained high by providing an initial oral fluid load of 500 to 800 mL water/m2 and replacing urine output with intake of water (mL for mL). First, some children may not be toilet trained and are unable to provide accurate collections of timed urine. Technical difficulties encountered in performing inulin infusions, reaching a steady state of inulin distribution, and accurately measuring inulin concentrations in plasma are added concerns. In addition, the inulin assay is not very specific, and it can be potentially hazardous (boiling acid reagents). These problems have rendered the standard inulin clearance impractical for use in children. Therefore, it is possible to determine the plasma clearance by infusing the substance at a constant rate until a steady state is achieved. Glomerular filtration rate / Clinical assessment of glomerular filtration rate 49 this constant infusion technique has used inulin, although other markers, especially radionuclide tagged tracers, also can be used (discussed later). After equilibration of the marker in its distribution space, the excretion rate equals the infusion rate. The renal clearance of the molecule can then be calculated from the rate of infusion and the concentration in plasma. The relative constancy of Cr production and its urinary excretion in the steady state helps one analyze for completeness of the collection.
600mg motrin with mastercard
There was no difference in adverse events or hematoma expansion between groups (Anderson et al pain management utica buy cheap motrin 400 mg. Enrollment has been completed but results are not available at the time of this writing (Qureshi and Palesch treatment for shingles pain and itching buy motrin 400mg low price, 2011). Rapid-sequence intubation is often pursued due to the risk of early neurologic decline and is appropriate when consciousness is threatened. Propofol and etomidate are preferred induction agents in this setting due to their relatively short half-lives (Diringer, 1993; Lummel et al. Dextrose-containing solutions should be avoided, considering the association of hyperglycemia with worse outcomes (Passero et al. However, this technology is only beginning to become available in a very few cities worldwide. Early arterial line placement for close blood pressure monitoring is frequently required for careful titration of antihypertensive therapy (Honner et al. Antiplatelet agents as well as platelet deficiency and dysfunction may also create a coagulopathic state (Hemphill et al. This suggests that aggressive intervention for both elevated blood pressure and coagulopathy correction may interact to limit hematoma expansion more than either intervention 184 A. This also sets a time benchmark for coagulopathy reversal that is reasonable to target. The efficacy and safety of idarucizumab, a monoclonal antibody directed against dabigatran, were recently evaluated in a prospective cohort study of 90 patients with serious bleeding or requiring an urgent procedure. Regarding antiplatelet agents, studies have found differing results regarding their impact on hematoma expansion and clinical outcome (Broderick, 2009; Naidech et al. Although current studies have failed to show improved outcomes with controlled normothermia in this setting (Broessner et al. However, the concern has been raised that aggressive treatment of elevated blood glucose may lead to systemic or cerebral hypoglycemia and potentially worsen outcomes (Vespa et al. Current guidelines recommend close monitoring of the glucose level and avoiding either hyperglycemia or hypoglycemia (Hemphill et al. However, the specific optimal target glucose and whether continuous insulin infusions should be used remain unclarified. Though there are no randomized clinical trials confirming these findings, there is generally not considered to be equipoise as to whether cerebellar surgery in these patients is beneficial. Several small studies have compared the efficacy of different techniques of minimally invasive hematoma evacuation to craniotomy, suggesting better outcomes with minimally invasive techniques (Cho et al. There was no difference in functional outcome, mortality, or the rate of infection (Naff et al. As of this writing, it has completed enrollment but results have not been reported. Additionally, physicians often desire to use initial prognostic models as a way of considering triage for ongoing care decisions. Perception of a poor prognosis without possibility of good recovery may lead to a decision to limit care or withdraw medical support. However, there is also the possibility that early care limitations may allow patients to die who would otherwise have the potential for an acceptable outcome. This leads to the possibility that withdrawal of care could lead to a self-fulfilling prophecy of poor outcome (Becker et al. It is thus considered imperative that rehabilitation begin as soon as possible for functional recovery. Multidisciplinary care of stroke patients has been proven to improve outcomes and to be cost-effective. This includes comprehensive stroke units, which can provide inpatient rehabilitation services before discharge, and home-based rehabilitation services, which can help accelerate hospital discharge and patient recovery (Outpatient Service Trialists, 2003; Chan et al.
Purchase motrin 600mg line
Mechanism underlying early anaemia in children with familial juvenile nephronophthisis back pain treatment yoga cheapest motrin. Familial clustering of medullary sponge kidney is autosomal dominant with reduced penetrance and variable expressivity kidney pain treatment natural discount motrin 400 mg with amex. Renal cysts and diabetes syndrome resulting from mutations in hepatocyte nuclear factor-1beta. What association exists between hypertension and simple renal cyst in a screened population Single-session percutaneous ethanol sclerotherapy in simple renal cysts in children: Long-term follow-up. Conservative and radiological management of simple renal cysts: A comprehensive review. Cystic nephroma and localized renal cystic disease in children: Diagnostic clues and management. Magnetic resonance imaging assessment of a murine model of recessive polycystic kidney disease. Volume progression in autosomal dominant polycystic kidney disease: the major factor determining clinical outcomes. Therapeutic potential of vasopressin V2 receptor antagonist in a mouse model for autosomal dominant polycystic kidney disease: Optimal timing and dosing of the drug. All of the conditions below are included in hepatocellular fibrocystic disorders, except: a. Small, contracted kidneys are characteristically seen in seen in which of the following cystic disease(s) A causal relationship between hypertension and renal cystic disease has been proposed in each of the following disorders except: a. Ciliopathies are a relatively new class of disorders, in which the pathologic process lies in the cilium and basal body complex. Interest in the cilium as an organelle, described in 1675 by Anthony van Leeuwenhoek, has gathered such momentum that a new journal dedicated to the cilia and its associated diseases was launched in 2012. It functions as a cellular antenna through which it allows the cell to remain constantly in contact with its environment. Ciliopathies result from mutation in genes encoding component proteins of the basal body, transition zone, or ciliary axoneme. The various signaling cascades intimately related to the primary cilium are discussed later. The result of these abnormalities is not only renal tubular cell dysfunction and renal cyst formation, but also abnormal development and organ function throughout the body. The cilium is assembled by the transfer of actin subunits from the cytoplasm by transport proteins. There are approximately 600 proteins within the cilium and their transport in and out of the cilium is closely regulated by specific ciliary localization sequence. The cilium transduces signals into the cell by the Sonic hedgehog and Wnt signaling pathways. The mother centriole is the older of the two and provides a template for the nine microtubule doublets to form the ciliary axoneme. The transition fibers and transition zone form a ciliary gate that mediates entry and exit of molecules into the cilium. In the absence of the ligand Sonic hedgehog (Shh), Patched (Ptch) represses the function of Smoothened (Smo) and there is no activation of Gli transcription factor. At the ciliary tip, Smo promotes activation of Gli (GliA), which enters the nucleus and promotes Hh-dependent gene transcription. Excess Sonic hedgehog (Shh) pathway activation can lead to severe developmental defects, extra digits, and tumor formation. When Shh binds to its receptor Ptch, Smo enters the cilium and induces activation of Gli3, which then translocates to the nucleus, where it regulates gene expression. A review of the ciliary signaling pathways mentioned previously and novel pathways such as the Hippo pathway can be found in a recent paper by Basten and Giles.
References: