Purchase uroxatral 10mg fast delivery
In this factorial design study prostate removal and sexual health discount 10mg uroxatral otc, patients received concurrent chemotherapy (weekly doses of carboplatin and paclitaxel) and cetuximab or placebo mens health belly off buy discount uroxatral 10mg on-line, followed by consolidation treatment. Patients who received higher radiotherapy dose had significantly worse survival (median of 20. Potential reasons for the unexpected results may lie in under-reported toxicity and in too-tight target volume margins in the high dose arm of the study. A considerable number of institutions continue to use higher total radiotherapy doses of 66Gy, often exceeding 2 Gy per fraction (hypofractionation), sometimes with simultaneous integrated boost technique. In patients who are not eligible for concurrent radiochemotherapy due to age or comorbidities, sequential chemotherapy and radiation remains the best option. Those who are not eligible for chemotherapy should be treated with definitive radiotherapy alone. A small, but significant, advantage for accelerated schedules was observed with a 2. Significantly better loco-regional outcomes were associated with highly accelerated schedules, emphasizing the importance of overall treatment time. Sequential schedules with highly accelerated radiotherapy are considered as important clinical research strategies to overcome the limitations of concurrent treatment. Therapy is individualized based on histological subtype, molecular pathology, age, comorbidities, expected toxicity, and patient preferences. Management of patients with non-small cell lung carcinoma not characterized by a genetic driver alteration First-line chemotherapy Chemotherapy prolongs survival as compared to best supportive care, with a meta-analysis reporting a 27% relative reduction in the risk of death equivalent to a 10% improvement in one year survival [69, 70]. Platinum-based combination chemotherapy is considered the standard of care in first-line treatment for patients with good performance status. Three meta-analyses evaluating the role of platinum-based vs platinum-free doublets reported a benefit in one-year survival in favour of platinum-based doublets, albeit of marginal statistical significance. This benefit was shown to be restricted to cisplatin in one analysis, and was absent when platinum-based doublet regimens were compared to third generation platinum-free doublets in another study. Three meta-analyses have shown a higher response rates for cisplatin when compared with carboplatin combinations. In the subset analysis, significantly superior efficacy was noted in the subgroup of non-squamous tumours and in patients treated with third generation cytotoxics. The largest trial comparing different platinum-based doublet regimens (cisplatin-paclitaxel, cisplatin-gemcitabine, cisplatin-docetaxel, carboplatin-paclitaxel) failed to demonstrate any difference in response or survival among the four arms [66]. To date, there is no definite clinical parameter or biomarker helping to identify patients at risk of rapid progression that would potentially benefit more from a maintenance strategy. Maintenance therapy should not be offered to patients with a performance status of 2 or greater or with persistent chemotherapy-induced toxicity. Furthermore, despite the low rate of grade 3 or 4 toxicities during maintenance treatment, the prolonged exposure of patients to grade 1 or 2 toxicities may be of significant concern. Prolongation of treatment, however, was also associated with a higher rate of adverse events and possible impairments of health-related quality of life [81]. In an attempt to improve the results of first-line combination therapy administered for a standard number of cycles, several maintenance strategies have been tested, either continuing one agent previously administered as first-line (continuation maintenance) or commencing an agent with a different mechanism of action (switch maintenance). Maintenance therapy is given without treatment-free period after the completion of first-line chemotherapy. In patients with performance status of 2, combination therapy of carboplatin and pemetrexed offers a significant survival advantage over pemetrexed alone [96]. Bevacizumab treatment is associated with a higher risk of thrombosis, hypertension, bleeding, proteinuria, and pulmonary haemorrhage [100].
Buy uroxatral 10 mg fast delivery
Current studies have shown the superiority of this modification with respect to operation time and intraoperative blood loss androgen hormones in females purchase cheap uroxatral on-line, while maintaining equal morbidity and short- and long-term mortality rates [96] prostate cancer news buy generic uroxatral 10 mg. Any suspicious areas will be biopsied and analysed by a pathologist via frozen sections to exclude systemic disease. The next step is the mobilization of the right colonic flexure, the duodenum, and pancreatic head by a Kocher manoeuvre. After dissection of the gastrocolic ligament or the greater omentum from the transverse colon, access to the lesser sac is obtained. Careful preparation of the hepatoduodenal ligament will provide details about potential arterial involvement and any potential accessory hepatic arteries. Left resection (pancreatic tail resection) Resection of the pancreatic tail will be performed in tumours of the left side and pancreatic corpus. The lower resection rate in this type of surgery results from the usually more advanced disease in left-sided pancreatic cancer, as symptoms usually only appear in a very late (unresectable) stage of disease. In most cases a splenectomy with resection of the splenic vessels will be performed simultaneously to achieve R0 status. After transection of the splenic artery and vein the pancreatic tail can then be removed together with the spleen; care should be taken to obtain a negative retroperitoneal resection margin. A recent trial has compared closure with a stapling device compare to hand suture and found no significant difference with regard to the fistula rate [92]. Total pancreatectomy If a clear resection margin cannot be achieved with a Whipple procedure or for multifocal tumours in the pancreas, a total pancreatectomy might be indicated if R0 resection status can then be achieved. En bloc venous resections can be performed with equal perioperative mortality and morbidity rates as standard resections. Median survival after venous resection is superior to palliative chemotherapy, and long-term survival is a possibility. Laparoscopic pancreatic surgery In recent years laparoscopic pancreatic surgery has evolved in some high-volume centres. Indications should be reviewed critically and laparoscopic surgery for pancreatic malignancies should be performed within clinical trials in high-volume centres only. Delayed gastric empting is a common morbidity after pancreatic surgery and describes the inability to return to normal diet after surgery. The patency of the pancreatic anastomosis (gastrojejunostomy or duodenojejunostomy) should be investigated endoscopically and a retropancreatic abscess should be excluded by abdominal cross-section imaging after prolonged times of delayed gastric emptying. Resection of arterial structures is technically feasible; however, its potential benefits are controversially discussed. A recent meta-analysis has shown that arterial resections are associated with an increased risk of perioperative mortality and poor one- and three-year survival rates. However, the results were still more favourable compared to no resection in advanced cases [106]. There have been documentations of small series for advanced disease within the corpus/cauda with extended pancreatic left resections plus splenectomy, gastrectomy, and celiac trunk resections (Appleby operation) [107]. Long-term outcome Pancreatic cancer, even when resected completely, is known for its dismal prognosis. The overall five-year survival rate for all patients is about 6% [125]; after resection the five-year survival rate approaches 20%. In the subgroup of patients without any adverse prognostic factor a five-year survival of 55% was observed in a recent study, whereas in subgroups of patients with more risk factors less favourable outcome was observed [126].
Order cheap uroxatral online
What surgical resection margins are required to achieve oncological control in men with primary penile cancer Distal urethral reconstruction of the glans for penile carcinoma: results of a novel technique at 1-year follow up prostate where is it located buy cheap uroxatral 10 mg line. Concomitant ventral phalloplasty during penile implant surgery: a novel procedure that optimizes patient satisfaction and their perception of phallic length after penile implant surgery man health news za discount uroxatral online. The results of primary radiation therapy in the management of squamous cell carcinoma of the penis. Surgical treatment of invasive squamous cell carcinoma of the penis: retrospective analysis of 350 cases. Squamous cell carcinoma of the penis: accuracy of tumour, nodes and metastasis classification system, and role of lymphangiography, computerized tomography scan and fine needle aspiration cytology. Contemporary morbidity from lymphadenectomy for penile squamous cell carcinoma: the M. Prospective validation of the association of local tumour stage and grade as a predictive factor for occult lymph node micrometastasis in patients with penile carcinoma and clinically negative inguinal lymph nodes. Tumour stage, vascular invasion and the percentage of poorly differentiated cancer: independent prognosticators for inguinal lymph node metastasis in penile squamous cancer. Corpus cavernosum invasion and tumour grade in the prediction of lymph node condition in penile carcinoma. A randomized comparison of sentinel node biopsy with routine axillary dissection in breast cancer. A new treatment for penile conservation in penile carcinoma: a preliminary study of combined laser hyperthermia, radiation and chemotherapy. Total glans resurfacing for premalignant lesions of the penis: initial outcome data. Glans resurfacing for the treatment of carcinoma in situ of the penis: surgical technique and outcomes. Prognostic factors of survival: analysis of tumour, nodes, and metastatic classification system. Penis conserving treatment for T1 and T2 penile carcinoma: clinical implications of a local recurrence. Magnetic resonance imaging combined with artificial erection for local staging of penile cancer. Current status of dynamic lymphoscintigraphy and sentinel lymph node biopsy in urological malignancies. Reliability and safety of current dynamic sentinel node biopsy for penile carcinoma. Two-center evaluation of dynamic sentinel node biopsy for squamous cell carcinoma of the penis. Dynamic sentinel lymph node biopsy in patients with invasive squamous cell carcinoma of the penis: a prospective study of the long-term outcome of 500 inguinal basins assessed at a single institution. Patients with penile carcinoma benefit from immediate resection of clinically occult lymph node metastases. Accuracy of sentinel lymph node biopsy for inguinal lymph node staging of penile squamous cell carcinoma: systematic review and meta-analysis of the literature. Contemporary management of regional nodes in penile cancer: improvement of survival Population-based survival of penile cancer patients in Europe and the United States of America: no improvement since 1990. Incidence trends and survival of penile squamous cell carcinoma in the Netherlands. The basaloid cell is the best tissue marker for human papillomavirus in invasive penile squamous cell carcinoma: a study of 202 cases from Paraguay. Combination chemotherapy with methotrexate, bleomycin and cisplatin for advanced squamous cell carcinoma of the male genital tract. Neoadjuvant chemotherapy followed by aggressive surgical consolidation for metastatic penile squamous cell carcinoma. Epidermal growth factor-related peptides and their receptors in human malignancies. Prognostic factors in patients with metastatic germ cell tumours who experienced treatment failure with cisplatin-based first-line chemotherapy.
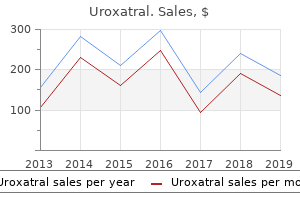
| Comparative prices of Uroxatral |
| # | Retailer | Average price |
| 1 | Whole Foods Markets | 124 |
| 2 | Office Depot | 259 |
| 3 | Giant Eagle | 448 |
| 4 | Bed Bath & Beyond | 549 |
| 5 | H-E-B | 362 |
| 6 | Ace Hardware | 345 |
| 7 | Limited Brands | 297 |
| 8 | IKEA North America | 532 |
Discount 10mg uroxatral mastercard
Neutrophils die after ingesting a small number of bacteria; the mixture of dead neutrophils prostate cancer 61 generic uroxatral 10mg online, other cells prostate cancer etiology purchase 10mg uroxatral visa, and fluid that can accumulate is called pus. Nerve cell endings are stimulated by direct damage and by some chemical mediators to produce pain sensations. In addition, the increased pressure in the tissue caused by edema and pus accumulation can cause pain. Pain, limitation of movement resulting from edema, and tissue destruction all contribute to the disturbance of function, which can be adaptive because it warns the person to protect the injured area from further damage. Chronic Inflammation Chronic, or prolonged, inflammation results when the agent responsible for an injury is not removed or something else interferes with the healing process. Infections of the lungs or kidneys usually result in a brief period of inflammation followed by repair. However, prolonged infections, or prolonged exposure to irritants, can result in chronic inflammation. Chronic inflammation caused by irritants, such as silica in the lungs, or abnormal immune responses can result in the replacement of normal tissue by fibrous connective tissue. Consequently, chronic inflammation of organs, such as the lungs, liver, or kidneys, can lead to death. When the inflammatory response lasts longer or is more intense than is desirable, drugs are sometimes used to suppress the symptoms by inhibiting the synthesis, release, or actions of the chemical mediators of inflammation. For example, medications called antihistamines suppress the effects of histamine released in people with hay fever. Aspirin and related drugs, such as ibuprofen and naproxen, are effective anti-inflammatory agents that relieve pain by preventing the synthesis of prostaglandins and related substances. Predict 6 In some injuries, tissues are so severely damaged that cells die and blood vessels are destroyed. For injuries such as these, where do the signs of inflammation, such as redness, heat, edema, and pain, occur In regeneration, the new cells are the same type as those that were destroyed, and normal function is usually restored. In fibrosis, or replacement, a new type of tissue develops that eventually causes scar production and the loss of some tissue function. The tissues involved and the severity of the wound determine the type of tissue repair that dominates. Regeneration can completely repair some tissues, such as the skin and the mucous membrane of the intestine. Stem cells are self-renewing, undifferentiated cells that continue to divide throughout life. With each division, there is a daughter stem cell and a second cell that can undergo differentiation. Regeneration can also involve division of differentiated cells in connective tissue and glands, such as the liver and pancreas. These cells do not normally divide, but retain the ability to divide after an injury. In the adult brain, heart, and skeletal muscle there are relatively few stem cells and the mature neurons, cardiac muscle, and skeletal muscle do not divide. While these cells cannot divide, they can recover from a limited amount of damage. For example, if the axon of a neuron is damaged, the neuron can grow a new axon, but it will die if the cell body is sufficiently damaged. Although neurons cannot form additional neurons, a small population of stem cells has been found in the adult brain. It may be possible to develop treatments for some brain injuries that stimulate the stem cells. Researchers have identified a class of chemicals, called growth factors, that stimulate stem cells to divide and make injured neurons recover more rapidly. The new neurons may be incorporated with other functional neurons of the central nervous system. In addition to the type of cells involved, the severity of an injury can influence whether repair is by regeneration or fibrosis. Generally, the more severe the injury, the greater the likelihood that repair involves fibrosis.
Discount 10mg uroxatral free shipping
It is rarely possible to make a prospective radiological diagnosis of a supratentorial ependymoma since their imaging features overlap significantly with those of a number of other lesions including glioblastoma prostate cancer 3rd stage proven uroxatral 10mg, ganglioglioma man health customer service cheap uroxatral 10 mg without a prescription, and pleomorphic xanthroastrocytoma. There is no clear evidence that prophylactic spinal irradiation prevents isolated spinal metastases, particularly if the primary tumour remains uncontrolled. The consensus view is that ependymomas should be treated with local irradiation to the site of the tumour and the appropriate margin, regardless of tumour grade and site. The technique and doses used are the same as those employed for other low-grade gliomas (54 Gy in 1. The prognosis is related to the histological grade, the extent of surgical resection, patient age, and performance status [136]. The presence of three or more risk factors determines a higher risk group with a median survival of three years. Glial tumours may involve any of the structures from the thalamus and hypothalamus through the midbrain to the pons and medulla. Just under 10% of cases are focal tectal glioma, often presenting with hydrocephalus, and prognosis exceeds ten years without irradiation [135]. Patients with medulloblastoma may present with raised intracranial pressure (usually due to hydrocephalus), cerebellar signs, and occasionally brainstem cranial nerve palsies. Medulloblastomas are usually solid, well-circumscribed intra-axial lesions of the cerebellum. Contrast enhancement is variable with some tumours enhancing avidly and relatively uniformly while some show only patchy enhancement and a small minority show no enhancement at all. Subarachnoid dissemination in the intracranial and spinal canal is a frequent finding. A medulloblastoma is approached by posterior fossa craniotomy and usually removal of the posterior arch of C1. The approach depends on the anatomical location of the tumour but the telovelar approach is the best choice for tumours in the fourth ventricle and avoids post-operative mutism [138]. In adults, 75% of ependymomas arise within the spinal canal, and up to 10% of patients have spinal metastases. Patients are classified according to extent of disease using the Modified Chang criteria [147]. The use of adjuvant chemotherapy in paediatric medulloblastoma has been extensively tested in sequential intergroup studies; however, there have been no trials in adults. As the natural history of adult medulloblastoma is similar to that in children, similar indications for chemotherapy could be accepted. The extent of disease defined by the Modified Chang criteria, age, completeness of resection, histological subtype, and genetic markers are prognostic indicators [150]. Stem cell transplant results in a disease-free survival in 24% of patients at ten years [152]. Tumours arising from the pineal gland can be germ cell tumours, pineal cell tumours, and gliomas (see Table 56. Due to their location, obstruction of the cerebral aqueduct with obstructive hydrocephalus is a common complication. Other features reflect the involvement of adjacent structures, such as the midbrain, hypothalamus, and the brainstem. Pineal germ cell tumours, like their systemic testicular counterparts, may secrete alpha-fetoprotein and human chorionic gonadotrophin into the cerebrospinal fluid and systemic circulation.
Order uroxatral 10mg amex
The other significant tumour factor relates to the presence of extrahepatic disease and vascular involvement which contraindicate resection androgen hormone feed loop buy 10 mg uroxatral fast delivery, transplantation prostate cancer 8-10 order uroxatral pills in toronto, or loco-regional therapies. Many patients are not amenable for curative treatment and benefit from palliative approaches with loco-regional or systemic therapies. While there is always a risk of recurrent disease in immunosuppressed post-transplant patients, the development of stringent criteria to select patients for transplantation reduces that risk. The widely used Milan criteria have been shown to give good outcomes, with five-year survival in excess of 70% post-transplant [101]. Milan criteria constitute a cirrhotic liver with a single lesion 5 cm or three lesions all 3 cm with no involvement of the portal vein and no extrahepatic disease [101]. Extended criteria have been developed that appear to have similar outcomes when considering long-term survival. While this study did not compare those within Milan criteria to those outside of it, the overall survival was comparable [102, 103]. A caution to increasing the criteria beyond Milan has also been raised regarding the availability of organs for non-malignant indications. The liver has distinct attributes that allow targeted treatment, and there is considerable interest in the synergistic effect of systemic chemotherapy and targeted liver treatments for liver dominant disease. Even with significant extrahepatic disease burden, it is disease progression in the liver that determines survival. Tumours up to 3 cm in maximal diameter are ablated with very low rates of residual disease leading to tumour recurrence [108]. Thermal ablative technologies such as radiofrequency ablation, laser, microwave, and cryoablation have all become established in routine practice. Catheter delivered treatment the portal vein provides in excess of 80% of the blood supply to the normal liver, while the hepatic artery is the main supply to both primary and secondary liver tumours. This situation can be exploited when targeting tumours with trans-arterial drug-delivery systems. The venous outflow via the hepatic veins into the inferior vena cava can be occluded. Technique Arterial access is usually via the common femoral artery, after which the coeliac and superior mesenteric arteries are imaged using a 4-5F catheter. A microcatheter (2-3F) is advanced within the 4F catheter to allow selection of the appropriate intrahepatic artery. If a solitary tumour is being treated then the catheter should be within the appropriate segmental artery, whereas if there is diffuse lobar disease the catheter is placed in the lobar artery. It is highly visible on fluoroscopy and persists in the malignant microvasculature, due to the lack of Kupffer cells. Either a resin or glass bead is used to carry yttrium 90, a -emitter, to the tumour capillary bed where it becomes trapped. The half-life of yttrium 90 is 64 hours which, combined with the short range of penetration, means that the patient poses little or no radiation risk to others in close proximity. Up to 50% of liver replacement by tumour is considered safe so long as the background liver function is satisfactory, and the portal vein patent [118, 119]. An initial arteriogram demonstrates the anatomy, especially vessels that may supply extrahepatic structures. It is very important to identify all such vessels as a single mal-deployed particle will cause tissue necrosis. Reflux of particles into these vessels is likely to lead to gastroduodenal ulceration or pancreatitis. High dose chemotherapy is then delivered to the whole liver via the hepatic artery. More than 90% of the chemotherapy is removed from the blood using a filtration and pump system, before being returned to the patient via an internal jugular vein sheath. The cytotoxic agent is bound to 30 um beads which do not to completely embolize the vessel supplying the tumour, but transport the cytotoxic agent to the tumour. The drug is then released into the surrounding tumour at a steady rate to ensure prolonged exposure and minimal systemic side effects [116, 117].
Buy generic uroxatral 10 mg on line
In cases of biochemical or clinical evidence of persistent/recurrent disease prostate 7 pill order uroxatral uk, reoperation would be the preferred treatment androgen hormone pills safe uroxatral 10mg. Radiation should be avoided until local disease is either symptomatic or rapidly progressing, and not amenable to reoperation. Radiation may be useful in treating symptomatic distant metastases, such as bone metastases. Localization and confirmation Imaging studies are recommended in patients with a basal calcitonin levels of 150 pg/ml (= 44 pmol/L) [12]. In patients having basal calcitonin levels <150 pg/ml (~ 44 pmol/L), the indication to perform imaging studies should be made on an individual basis. Due to the nature of C-cell metastasis (multiple, micronodular, involving the whole organ), laparoscopy has been successfully used to identify liver metastases [29]. Chemotherapy and other treatment modalities Some experimental studies with chemotherapy are promising. Currently, one of the best results has been achieved by combining dacarbazine, fluorouracil, and doxorubicin [12]. In animal studies, an improved efficacy was shown combining radioimmunotherapy and antiangiogenic therapy [33]. The great majority of adrenocortical tumours are benign and hormonally silent (non-functioning). Virilizing and feminizing tumours, probably arising from the zona reticularis, are more rare; however, tumours secreting combinations of adrenocortical steroids have also been described [39, 40]. Molecular-targeted therapy is most promising and we should expect new treatment options in the near future. Besides tumour stage, post-operative calcitonin level is the most powerful prognostic factor. A doubling-time of less than six months correlates with a poor prognosis while one more than two years correlates with a good prognosis. Adrenal adenomas may occur at any age; bilateral adenomas are rare, but occur as part of familial adenomas [39]. Follow-up Following surgery, all patients need lifelong replacement of levothyroxine (L-T4). In this respect, there is generally no difference between sporadic and hereditary cases. However, it is unknown whether screening patients who underwent prophylactic thyroidectomy and histologically only showed C-cell hyperplasia need to undergo follow-up at all. If either basal or stimulated calcitonin level is abnormal, further investigations may be indicated to localize the residual disease. If medical management is not altered as a response to calcitonin levels in individual cases, there is no need to subject the patient to repeated tests. Diagnosis and staging Patients with adrenal adenomas usually present with the gradual onset of symptoms and signs of hypercortisolism. The presence of proximal myopathy, vascular fragility, and thin skin can be used to clinically differentiate them from other pseudo-Cushingoid states [43]. Benign adenomas are usually pure cortisol secretors, and hirsutism and other androgenic effects are usually absent. However, components of the syndrome due to mineralocorticoid excess (hypertension, hypokalaemia) and virilization have been described. As a screening test, measurement of the 9 am serum cortisol after dexamethasone 1 mg at midnight has very high sensitivity but rather low specificity. Adrenal tumours Adrenocortical tumours the adrenal cortex comprises 90% of the normal adult adrenal gland and weighs up to 4 g. It consists of three zones: the outer zona glomerulosa (15% of the cortex), which expresses the enzyme 18-oxidase and can thus secrete aldosterone; the middle zona fasciculata (75% of the cortex); and inner zona reticularis which express the enzyme 17-hydroxylase and can secrete cortisol, androgens, oestrogens, and weak mineralocorticoids. The specimen is attached to the inferior vena cava, which has been opened as far as the right atrium and ventricle.
Buy discount uroxatral 10mg online
The blood lymphocyte count must be charted at diagnosis and at each follow-up to determine the doubling time man healthcom 2014 report discount 10mg uroxatral visa. Molecular changes leading to the pathogenesis of the disease are still poorly understood prostate biopsy results purchase uroxatral discount. Patients with 17p or 11q deletion generally have more advanced disease with frequent splenomegaly, mediastinal, and abdominal lymphadenopathy and more extensive peripheral lymphadenopathy. Chlorambucil is still indicated for use in the low-risk patient and elderly patients who have a poor performance status. The drug also suppresses both T and B lymphocytes with resultant increase in bacterial, viral and opportunistic infections [142, 143]. Treatment options are: (i) chlorambucil, (ii) fludarabine, (iii) fludarabine + cyclophosphamide, or (iv) observation. Selecting the best treatment for an individual patient is sometimes difficult and challenging. Patients either relapsing rapidly or not responding to first-line chlorambucil should be considered for fludarabine-containing regimens. The majority of patients treated with these agents and combinations have a partial response. Three randomized trials have shown the superiority of this combination over fludarabine alone. Even though the combination produces more myelosuppression, infection rates and mortality due infection have not been found to be increased. However, grade 3 and 4 neutropaenia have been reported in 51% patients [151, 152]. Grade 3/4 neutropaenia was significantly more common in the three-drug regimen [153, 154]. Combination of rituximab with purine analogues and/or alkylating agents significantly adds to activity and potency [152, 154, 156]. Rituximab administration can be associated with significant infusion toxicities including rigors, anaphylactic reactions, and hypotension. As a rule, premedication with steroids and antihistaminics should be given to all patients and the infusion should be initiated slowly under careful monitoring of vital parameters. The initial approval of the drug was for patients who were refractory to fludarabine [159] but recently it has been approved for first-line use also. There are some reports suggesting that alemtuzumab may have significantly more activity than standard treatment in high-risk patients who have 17p and 11q deletions [160, 162]. The drug has shown encouraging activity when combined with fludarabine [163, 164] and chlorambucil [162]. Subcutaneous administration of the drug is effective and is being tested in clinical trials [165, 166]. Management of the relapse/refractory chronic lymphocytic leukaemia patient the most important consideration in the choice of therapy for the patient who relapses is the initial treatment and the duration of response to the same. The drug is indicated either alone or in combination with fludarabine or rituximab. Rituximab in combination with purine analogues is being tested in relapsed patients. Infiltration in the spleen occurs exclusively in the red pulp with sparing of the white pulp, liver involvement is restricted to sinusoids, and lymph node infiltration is rare [187]. The fibrosis seen in the involved tissues is thought to be due to the secretion of fibronectin by the hairy cells, which is an extracellular matrix ligand for a4b.
References: