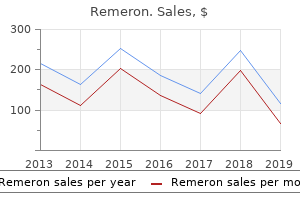
"Buy generic remeron on-line, treatment toenail fungus".
By: W. Thorus, M.A., M.D.
Co-Director, Rutgers Robert Wood Johnson Medical School
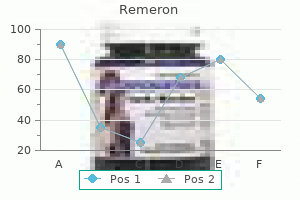
On the other hand symptoms 8dp5dt purchase remeron 30mg with visa, distention of the antrum treatment 4 ulcer cheap remeron 30 mg online, but not the fundus, with a balloon induces nausea sensations and gastric dysrhythmias in healthy individuals. Electrical recordings from electrodes secured to the mucosa of the proximal, middle, and distal antrum in a healthy subject. A, 3-cycle-per minute (cpm) electrical slow waves in the proximal, middle, and distal electrode leads. The slow waves are propagated in an aborad direction as indicated by the dotted lines. B, Disruption of propagation and the onset of a 5- to 6-cpm tachygastria in the distal lead during hyperglycemia (glucose clamping), with a blood glucose level of 240 mg/dL. Coupling and propagation of normal dysrhythmic gastric slow waves during acute hyperglycemia in healthy humans. Illusory self-motion (vection) induces antral hypomotility, tachygastria, and decreased gastric emptying. The vagus nerve contains afferent nerves with A-delta and C pain fibers with cell bodies in the nodose ganglia and connections to the nucleus tractus solitarius (not shown). Low threshold mechano- and chemoreceptors stimulate visceral sensations such as gastric emptiness or fullness and symptoms such as nausea and discomfort. These stimuli are mediated through vagal pathways and become conscious perceptions of visceral sensations if sensory inputs reach the cortex. The splanchnic nerves also contain afferent nerves with A-delta and C fibers that synapse in the celiac ganglia with some cells bodies in the vertebral ganglia (T5-T9). Interneurons in the white rami in the dorsal horn of the spinal cord cross to the dorsal columns and spinothalamic tracts and ascend to sensory areas of the medulla oblongata. These splanchnic afferent fibers are thought to mediate high-threshold stimuli for visceral pain. In contrast to visceral sensations, somatic nerves such as those from the skin carry sensory information via A-delta and C fibers through the dorsal root ganglia and into the dorsal horn and then through dorsal columns and spinothalamic tracts to cortical areas of somatic representation. Changes in gastric electrical rhythm, excess amplitude contractions, or stretch on the gastric wall are peripheral mechanisms that elicit changes in afferent neural activity (via vagal and/or splanchnic nerves) that may reach consciousness to be perceived as visceral perceptions (symptoms) emanating from the stomach. The ingestion of food elicits relaxation of the stomach musculature (receptive relaxation) and accommodation of the physical volume of the meal; as these gastric neuromuscular events occur, hunger disappears and the comfortable, postprandial sensations of stomach fullness are experienced. The volume of food ingested suppresses hunger and stimulates the sense of fullness more than the calorie content of the meal. The physiologic attributes of postprandial fullness are not completely known, but the physical stretch on the stomach walls (and changes in intragastric pressure) induced by ingestion of food and the secretion of gastric juice are in part responsible. The average volume of water ingested to achieve fullness is 600 mL; in contrast, patients with functional dyspepsia only ingest, on average, 350 mL to feel full, indicating a disturbance in stomach wall relaxation and/or wall tension. Gastric myoelectrical response to sham feeding with tasty food (A) and "disgusting" food (B). The increase in amplitude of the peaks in the normal 3-cycle-per minute (cpm) range during sham feeding is the normal response. Note the lack in increase of 3-cpm peaks during sham feeding the tofu dog compared with (A). On both days, the subject then ingested a warm hot dog on a bun at "Meal"; note the subsequent increase in peaks at 3 cpm. Sensations of fullness continue during the lag phase when the food is being triturated. Once the linear phase of gastric emptying begins, there is a progressive perception of decreasing stomach fullness and increasing stomach emptiness over time. Four or 5 hours after a solid meal, the stomach is indeed empty and the healthy individual feels hungry once again. The physiologic mechanisms of hunger and satiety (and stomach emptiness and fullness) are under intense investigation. The sight, smell, and taste of food stimulate central vagal efferent activity that increases gastric acid secretion, gastric contractility, and increases 3cpm gastric myoelectrical activity. Patients with unexplained nausea symptoms may have altered emptying of liquid meals, even if solid phase emptying is normal.
The ability of the clinician to elicit an accurate history of abdominal pain and peritoneal signs is limited in patients with neurologic and immunologic compromise medicine 600 mg buy discount remeron 15 mg online. Infants and children may be incapable of furnishing any history or cooperating with the physical examination treatment 8th february discount remeron 15mg with visa. Analgesics typically will not relieve the findings of peritonitis on physical examination, but may relieve some discomfort. In fact, it has been shown that early provision of analgesia to patients with undifferentiated abdominal pain does not affect diagnostic accuracy. Patients receiving immunosuppressive and anti-inflammatory drugs, such as glucocorticoids and chemotherapeutic drugs, may have blunted perception of pain and minimal signs of peritoneal irritation. In addition, metabolic acidosis, hemoconcentration, and prerenal azotemia may be present. Free air may be detected on upright chest radiograph or on upright or decubitus abdominal films, but the finding of pneumoperitoneum by radiography has limited sensitivity in gut perforation. The axial images are of extremely high resolution and can be reconstructed in coronal, sagittal, and 3-dimensional sets of images. Pressor therapy should be initiated only after adequate volume resuscitation has failed to correct hypotension and hypoperfusion. The use of glucocorticoids in the treatment of severe sepsis remains controversial. A recent meta-analysis of 20 clinical trials showed no conclusive reduction in mortality. Antibiotics Antibiotic therapy is required before, during, and after surgical intervention. Two recent sets of guidelines for the management of complicated intra-abdominal infections recommend broader antimicrobial therapy for hospital-acquired infections than in community-acquired infections. In general, antibiotics directed against the most likely pathogens should be chosen. For example, colonic processes require coverage for Gramnegative aerobes and anaerobes. In animal models, antibiotics directed against Gram-negative enteric aerobic organisms minimize mortality, and drugs effective against anaerobes prevent abscess formation. It has been shown that there is synergism between aerobic and anaerobic bacteria in experimental models of peritonitis. The flora of surgical peritonitis simplifies with time, even before initiation of antibiotics. Killing certain key species may change the microenvironment sufficiently to prevent growth and allow killing of other flora. If a Candida species is cultured from the peritoneal cavity, this organism should be treated if the patient is in septic shock, in an immunocompromised state, or in a hospital-acquired setting. For example, it has been shown that monotherapy with a broad-spectrum beta-lactam is as effective as combination therapy with a beta-lactam and an aminoglycoside. A recent Cochrane review of 40 randomized trials involving 16 different regimens showed no difference in mortality. The failure to clear secondary peritonitis after an appropriate course of antibiotic therapy or the recurrence of peritonitis Diagnosis the diagnosis of surgical peritonitis is suspected on the basis of history, physical examination, and laboratory and imaging tests and is confirmed at laparotomy or laparoscopy when purulent fibrinous peritonitis is found. Peritoneal lavage is performed by inserting a catheter under sterile conditions into the peritoneal cavity and infusing 1 L of normal saline. Finally, diagnostic laparoscopy is extremely accurate in making the diagnosis of surgical peritonitis and many of the underlying diseases can be dealt with laparoscopically, avoiding the need for laparotomy. The second principle is that the absence of peritonitis does not exclude the possibility of surgical emergency. The classic example of this clinical situation is early acute mesenteric ischemia with abdominal pain out of proportion to findings on physical examination findings (see Chapter 118). Likewise, a complete mechanical small bowel obstruction without peritoneal signs, an indication of perforation or vascular compromise, still requires operation (see Chapter 123). For most cases of secondary (surgical) peritonitis, fluid resuscitation and antibiotic therapy followed by urgent laparotomy or laparoscopy are the mainstays of treatment. The patient should be aggressively fluid resuscitated to treat intravascular fluid depletion secondary to movement of fluid out of the vascular space.
Syndromes
- Examination of the eyes
- Do you have other symptoms such as pain, nipple discharge, or fever?
- Standard eye exam
- Laser therapy called an iridotomy
- ECG
- Complete blood count (CBC), clotting tests, platelet count, and other laboratory tests
- Abdominal aortic aneurysm can cause a pulsating mass around the navel.
- Lack of periods in women (amenorrhea)
- Applying moist, warm compresses to the infected area
- Pain is persistent, unexplained, or accompanied by other unexplained symptoms. Call your primary health care provider.
Adequate well-controlled or observational studies in pregnant women have demonstrated a risk to the fetus medicine 018 purchase remeron online from canada. Adequate well-controlled or observational studies in animals or pregnant women have demonstrated evidence of fetal abnormalities symptoms nausea headache fatigue purchase 30mg remeron mastercard. The use of the product is contraindicated in women who are or may become pregnant. Hepatic Function During pregnancy, maternal blood volume increases progressively until week 30 of gestation when it is 50% greater than normal and remains so until confinement. Thus, total serum protein concentrations diminish 20% by mid-pregnancy, largely as a result of a reduced serum albumin level. Active transport may be involved in the transplacental movement of some macromolecules. Despite increases in maternal blood volume, the levels of many serum proteins measured to assess hepatic injury are unchanged or even increased during gestation. Progesterone causes a proliferation of smooth endoplasmic reticulum, whereas estrogens promote formation of rough endoplasmic reticulum and associated protein synthesis. Pregnant women synthesize the products of the cytochrome P-450 gene superfamily and other proteins at an accelerated rate, including coagulation factors, binding globulins, and ceruloplasmin. Maternal serum alkaline phosphatase levels normally are elevated during the third trimester of pregnancy, largely due to placental production; for this reason, measurement of alkaline phosphatase in pregnant women is only of clinical use early in gestation. Alterations in maternal concentrations of plasma proteins may persist for several months postpartum. Mild leukocytosis and increased erythrocyte sedimentation rates are also common in normal pregnancy. In the second and third trimesters, the supine position and external abdominal pressure should be avoided because resulting compression of the vena cava and aorta may cause hypotension and placental hypoperfusion. Sedation with benzodiazepines (pregnancy category D) should be avoided, especially during the first trimester, because diazepam has been reported to cause fetal malformations. Although nausea and vomiting may vary from mild to severe, most affected individuals still are able to obtain adequate oral nutrition and hydration, in some cases by eating frequent small meals of dry starchy foods. Severe persistent vomiting demanding medical intervention, or hyperemesis gravidarum, is less common, occurring in 2% or less of pregnancies. Symptoms usually begin at weeks 4 to 5 and improve by weeks 14 to 16 of gestation. Reported risk factors for hyperemesis include a personal or family history of the disorder,52 a female fetus or multiple gestation, gestational trophoblastic disease, fetal trisomy 21, hydrops fetalis, and maternal Hp infection. An increased risk of hyperemesis was found in a meta-analysis of case-controlled studies,62 whereas others could not establish any relationship between the 2 conditions. Contrast agents may cross the placenta, and their safety in pregnant women has not been formally assessed. Abnormal laboratory test results in such patients include hypokalemia, hyponatremia, and ketonuria. Hyperemesis is associated with slight increases in serum aminotransferase and bilirubin levels in 25% to 40% of cases. Hyperamylasemia, seen in a quarter of affected patients, is due to excessive salivary gland production stimulated by prolonged vomiting. In a study of more than 150,000 singleton pregnancies, infants born to women with hyperemesis who had gained less than 7 kg of weight during pregnancy were more likely to have low birth weights, be premature and small for gestational age, and to have low Apgar scores. Obstetric management should be overseen, if possible, by physicians qualified in maternal-fetal medicine. The goals of therapy are maintenance of adequate maternal fluid intake and nutrition, as well as symptom control. Patients should be advised to eat multiple small meals as tolerated and to avoid an empty stomach, which may trigger nausea. Also, avoidance of offensive odors, separation of ingestion of solid and liquid foods, and consumption of a high-carbohydrate diet may be helpful.
The prevalence of hereditary hemorrhagic telangiectasia in juvenile polyposis syndrome medications used to treat adhd generic remeron 30mg. Vascular endothelial growth factor serum levels are elevated in patients with hereditary hemorrhagic telangiectasia treatment sciatica purchase remeron discount. The liver in hereditary hemorrhagic telangiectasia: An inborn error of vascular structure with multiple manifestations. An angiographic study of abdominal visceral angiodysplasias associated with gastrointestinal hemorrhage. Brief report: Treatment of bleeding in hereditary hemorrhagic telangiectasia with aminocaproic acid. Bevacizumab reverses need for liver transplantation in hereditary hemorrhagic telangiectasia. Bevacizumab in patients with hereditary hemorrhagic telangiectasia and severe hepatic vascular malformations and high cardiac ouput. Bevacizumab as rescue treatment for severe recurrent gastrointestinal bleeding in hereditary hemorrhagic telangiectasia. Iron deficiency anemia related to hereditary hemorrhagic telangiectasia: Response to treatment with bevacizumab. Gastric antral vascular ectasia in cirrhotic patients: Absence of relation with portal hypertension. Treatment of chronic transfusion-dependent gastric antral vascular ectasia (watermelon stomach) with thalidomide. Efficacy of thalidomide for refractory gastrointestinal bleeding from vascular malformation. Gastric antral vascular ectasia causing severe hypoalbuminemia and anemia cured by antrectomy. Computed virtual chromoendoscopy-enhanced videocapsule endoscopy is of potential benefit in gastric antral vascular ectasia syndrome refractory to endoscopic treatment. Comparison of argon plasma coagulation in management of upper gastrointestinal angiodysplasia and gastric antral vascular ectasia hemorrhage. Treatment of gastropathy and gastric antral vascular ectasia in patients with portal hypertension. The effects of transjugular intrahepatic portosystemic shunt on portal hypertensive gastropathy. Effect of transjugular intrahepatic portosystemic shunt formation on portal hypertensive gastropathy and gastric circulation. Double-blind randomized, comparative multicenter study of the effect of terlipressin in the treatment of acute esophageal variceal and/or hypertensive gastropathy bleeding. Portal colopathy: Prospective study of colonoscopy in patients with portal hypertension. Dieulafoy lesions: A review of 6 years of experience at a tertiary referral center. Capillary hemangioma of the esophagus in a patient with systemic sclerosis and gastric antral vascular ectasia. Mechanisms, indications and results of salvage systemic therapy for sporadic and von Hippel-Lindau related hemangioblastomas of the central nervous system. Identification of an angiographic factor that when mutated causes susceptibility to Klippel-Trenaunay syndrome. Klippel-Trenaunay syndrome with gastrointestinal bleeding, splenic hemangiomas and left inferior vena cava. Bleeding from cavernous angiomatosis of the rectum in Klippel-Trenaunay syndrome: Report of three cases and review of the literature. Aneurysm stent graft versus open surgical repair of abdominal aortic aneurysms: Multicenter prospective clinical trial. Rare causes of occult small intestinal bleeding including aortoenteric fistulas, small bowel tumors and small bowel ulcers. Primary aortoenteric fistulae: the challenges in diagnosis and review of treatment.
The spectrum of pediatric eosinophilic esophagitis beyond infancy: A clinical series of 30 children treatment of shingles remeron 30mg mastercard. Significance of eosinophil and mast cell counts in rectal mucosa in ulcerative colitis medicine bg order remeron overnight delivery. Intraepithelial eosinophils in endoscopic biopsies of adults with reflux esophagitis. Primary eosinophilic esophagitis in children: Successful treatment with oral corticosteroids. Infiltration of peroxidase-producing eosinophils into the lamina propria of patients with ulcerative colitis. Reflux esophagitis: Sequelae and differential diagnosis in infants and children including eosinophilic esophagitis. Eosinophilic gastroenteritis: Immunohistochemical evidence for IgE mast cell-mediated allergy. Eosinophil gastroenteritis in extreme allergy: Immunopathological comparison with nonallergic gastrointestinal disease. Food allergy manifested by eosinophilia, elevated immunoglobulin E level, and protein-losing enteropathy: the syndrome of allergic gastroenteropathy. Elimination diet effectively treats eosinophilic esophagitis in adults; food reintroduction identifies causative factors. The chemokine eotaxin is a central mediator of experimental eosinophilic gastrointestinal allergy. A critical role for eotaxin in experimental oral antigen-induced eosinophilic gastrointestinal allergy. Eosinophilic infiltration of the esophagus: Gastroesophageal reflux versus eosinophilic esophagitis in children-Discussion on daily practice. Ringed oesophagus and idiopathic eosinophilic oesophagitis in adults: An association in two cases. Infiltrating eosinophils and eotaxin: Their association with idiopathic eosinophilic esophagitis. The physiological and pathophysiological roles of eosinophils in the gastrointestinal tract. Human eotaxin is a specific chemoattractant for eosinophil cells and provides a new mechanism to explain tissue eosinophilia. Approaches to the treatment of hypereosinophilic syndromes: A workshop summary report. Clinical, pathologic, and molecular characterization of familial eosinophilic esophagitis compared with sporadic cases. Interleukin-5mediated allergic airways inflammation inhibits surfactant protein C promoter in transgenic mice. Eosinophil infiltration of the oesophageal mucosa in patients with pollen allergy during the season. Epicutaneous antigen exposure primes for experimental eosinophilic esophagitis in mice. Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. Quality of life in paediatric eosinophilic oesophagitis: What is important to patients Prevalence and predictive factors of eosinophilic esophagitis in patients presenting with dysphagia: A prospective study. Association of eosinophilic inflammation with esophageal food impaction in adults. Treatment of eosinophilic esophagitis with specific food elimination diet directed by a combination of skin prick and patch tests. Esophageal eosinophilic infiltration responds to proton pump inhibition in most adults.
The mannose-6-phosphate groups serve as a recognition site for a specific receptor medicine clip art purchase genuine remeron. The interaction of the lysosomal enzyme mannose 6-phosphate with its receptor leads to formation of vesicles that transport this complex to the lysosome medications not to take with grapefruit discount remeron master card, delivering the enzyme. In the lysosome the enzyme dissociates from the receptor, which in turn cycles back to the Golgi complex. Trypsinogen, chymotrypsinogen, proelastase, procarboxypeptidase, and prophospholipase A2 are stored in the pancreas and secreted into the duodenal lumen as inactive proenzyme forms. There, the brush-border enzyme enterokinase converts secreted trypsinogen to trypsin. Trypsinogen and the other proenzymes are then converted to active forms by proteolytic cleavage by trypsin. Pancreatic acinar cell agonists that stimulate digestive enzyme secretion act through 2 separate pathways. That is, the observed response is greater than would be expected from the additive responses of the individual agonists acting alone. Gastrointestinal Teaching Project, American Gastroenterological Association; 2003. Regulation of Protein Synthesis the mechanisms involved in regulating expression of digestive enzymes in the exocrine pancreas have been partially elucidated. The investigations have addressed the following 2 questions: First, what accounts for the specific expression of digestive enzymes in the pancreas Second, how do alterations in dietary nutrients change the synthesis of specific digestive enzymes Regarding the second question, numerous studies have demonstrated that the relative synthesis rates of specific digestive enzymes change as a function of dietary intake. For example, a carbohydrate-rich diet results in an increase in synthesis of amylase and a decrease in that of chymotrypsinogen,47 a lipid-rich diet enhances lipase expression,48 and an alcohol-rich diet decreases amylase expression. Studies involving the use of human tissue are limited but emerging importantly in physiologic and pathophysiologic studies of the exocrine pancreas. Furthermore, the molecular structure for each of these receptor types has been elucidated from cloning and sequencing. The actions of these agonists include stimulating cellular metabolism of membrane phosphoinositides and raising intracellular free calcium Chapter 56 PancreaticSecretion 939 concentrations ([Ca2+]i) from mobilization of intracellular stores. The calcium release into the cytosol causes a rapid rise in the concentration of free calcium that is necessary for the secretory response. The continued stimulation of enzyme secretion by these agents also depends on the influx of extracellular calcium. The exact mechanism of this potentiated response is not known, but it probably functions physiologically so that significant quantities of secretion occur with a combination of small increases in individual agonists. Digestive Secretion Like gastric secretion, exocrine pancreatic secretion with ingestion of a meal is divided into 3 phases: cephalic, gastric, and intestinal. The extent of cephalic stimulation of exocrine pancreatic secretion in humans has been evaluated through measurement of exocrine secretions stimulated by sham feeding (chewing and spitting out the food). One study70 indicated that sham feeding stimulated pancreatic enzyme secretion at up to 50% of the maximal secretory rate, with no increase in bicarbonate secretion when acidic gastric secretions were prevented from entering the duodenum. When gastric secretions were allowed entry into the duodenum, the rate of pancreatic enzyme secretion rose to about 90% of maximal, and bicarbonate was also secreted. These results suggest that cephalic stimulation specifically stimulates acinar secretion in the pancreas, and that a low pH in the duodenum (from gastric acid) augments acinar secretion as well as causes ductal bicarbonate secretion. The major stimulus is gastric distention, which causes predominantly secretion of enzymes with little secretion of water and bicarbonate. Balloon distention of either the gastric fundus or the antrum results in a low-volume, enzyme-rich secretion by way of a gastropancreatic vagovagal reflex. Three gastric processes- secretion of acid, pepsin, and lipase; digestion; and emptying- are tightly coupled to the mechanisms of the intestinal phase of pancreatic secretion. The intestinal phase begins when chyme first enters the small intestine from the stomach.
Phosphate Salts. Remeron.
- How does Phosphate Salts work?
- Low blood phosphate, when sodium and potassium phosphates are used.
- Sensitive teeth, heartburn, cleaning out the bowels as a laxative preparation for intestinal tests such as colonoscopy when sodium phosphates are used, and other conditions.
- Are there safety concerns?
- Improving aerobic exercise performance.
- Dosing considerations for Phosphate Salts.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96719
Surgical mortality is higher if the inflammatory mass occludes or compresses major arteries or veins symptoms 1 week after conception generic remeron 30mg overnight delivery. In 1 modification developed by Frey medication 3 checks buy cheap remeron 30 mg, less of the head of the pancreas is cored out, leaving the bile duct and peripancreatic vessels undisturbed. A third operation, the Berne procedure, uses a pancreatic head resection without longitudinal duct incision, but leaves a narrow layer of pancreatic tissue against the duodenum and retropancreatic vessels. Surgical options for pain are pancreatic ductal drainage, resection of all or part of the pancreas, and both. The choice of surgical procedure depends in large part on the ductal anatomy, presumed pathogenesis of pain, and associated complications, as well as local surgical preferences and expertise. The rationale for these procedures is to relieve ductal obstruction and reduce pancreatic pressures, thereby relieving pain. Pancreatic ductal drainage procedures generally require dilation of the pancreatic duct to more than 6 or 7 mm, a diameter that allows relatively easy identification and anastomosis. The most commonly performed procedure is the lateral pancreaticojejunostomy or PartingtonRochelle modification of the Puestow procedure. In this procedure, the pancreatic duct is opened longitudinally and anastomosed to a defunctionalized limb of small bowel, which is connected with a Roux-en-Y anastomosis. At the time of the operation, ductal strictures can be incised and stones can be readily removed as needed. The procedure also can be performed in the absence of a dilated pancreatic duct (normal duct Puestow procedure), but the efficacy for relieving pain is believed to be less. The explanation for this decline in effectiveness is unknown but may reflect closure of the anastomosis, pain originating in the undrained segments of the head of the pancreas, or the development of other sources of pain. There is thus a tradeoff between the simplicity and low risk of this procedure and the gradual decline in pain relief over time. Exocrine and endocrine functions are generally unaffected by this surgical procedure per se, but appear to continue to deteriorate as in unoperated patients. In an attempt to overcome the modest early and substantial late failure rates of simple drainage procedures, approaches combining resection of the pancreas with drainage Chapter 59 ChronicPancreatitis 1019 undergoing Whipple procedures. One meta-analysis noted that the Beger operation may be somewhat superior in terms of pain relief, whereas the Frey variation may have less postoperative morbidity314 compared to a Whipple operation. Randomized trials comparing the Beger with the Frey operations, however, show similar rates of postoperative complications, efficacy, and long-term quality of life. Postoperative complications are more common than with a simple modified Puestow procedure, but both short- and long-term pain relief is superior. Laparoscopic and robotic-assisted approaches are possible for most of these technically challenging operative approaches. In some patients with disease limited to the body and tail of the pancreas, typically after trauma to the pancreatic duct in the body of the pancreas with upstream obstructive chronic pancreatitis, resection of the body and tail may be considered. In patients with a nondilated pancreatic duct, a small V-shaped excision can be performed on the ventral surface of the pancreas over the pancreatic duct with an overlying pancreaticojejunostomy (similar to a modified Puestow operation) with acceptable results. In practice, insulin independence is achieved in about 40% of patients, with pain relief in 80% to 90% of patients. They include pancreatic fistula, wound infection, delayed gastric emptying, intra-abdominal abscess, pancreatitis, cholangitis, and bile leak. Exocrine insufficiency in particular may escape detection because symptoms may be mild. Steatorrhea can develop in 30% to 40% of patients undergoing simple drainage procedures and in up to two thirds of those undergoing pancreatic resections. The development of endocrine insufficiency after pancreatic surgery is also common but not invariable, and some series have even noted improvements in glucose tolerance in some patients after surgery. In general, however, diabetes mellitus still commonly occurs after surgery either as a consequence of pancreatic resection or from the ongoing ravages of the disease. Nerve Blocks and Neurolysis the celiac plexus transmits visceral afferent impulses from the upper abdominal organs, including the pancreas. The greater, lesser, and least splanchnic nerves travel from the celiac plexus and then pass through the diaphragm to reach the spinal cord. Attempts to block the transmission of nociceptive stimuli have met with limited success.
Alendronate-induced esophagitis: Case report of a recently recognized form of severe esophagitis with esophageal stricture: Radiographic features symptoms vertigo discount 30mg remeron otc. Placebo-controlled symptoms whooping cough purchase cheap remeron, randomized, evaluator-blinded endoscopy study of risedronate vs. Oesophageal transit, disintegration and gastric emptying of a film-coated risedronate placebo tablet in gastro-oesophageal reflux disease and normal control subjects. Nitrovasodilators, low-dose aspirin, other nonsteroidal anti-inflammatory drugs, and the risk of upper gastrointestinal bleeding. Fatal esophageal and bronchial artery ulceration caused by solid potassium chloride. A case of esophageal perforation due to a pill-induced ulcer successfully treated with conservative measures. Paracetamol-induced perforation of the esophagus in a patient with eosinophilic esophagitis. Vincristine-induced dysphagia suggesting esophageal motor dysfunction: A case report. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices. Perforation of esophagus after endoscopic variceal sclerotherapy: Incidence and clues to pathogenesis. Effect of endoscopic variceal sclerotherapy on esophageal motor functions and gastroesophageal reflux. Spontaneous rupture of iatrogenic intramural hematoma of esophagus during endoscopic sclerotherapy. Development of early squamous cell carcinoma of the esophagus after endoscopic injection sclerotherapy for esophageal varices. Sequelae after esophageal variceal ligation and sclerotherapy: A prospective randomized study. Sequential esophageal motility studies after endoscopic injection sclerotherapy: A prospective investigation. Prevention of stricture formation after endoscopic sclerotherapy of esophageal varices. Prophylactic administration of ranitidine after sclerotherapy of esophageal varices. Role of omeprazole in prevention and treatment of postendoscopic variceal sclerotherapy esophageal complications: Double-blind randomized study. Nasogastic intubation causes gastroesophageal reflux in patients undergoing elective laparotomy. The effect of nasogastric intubation on gastroesophageal reflux: A comparison of different tube sizes. Esophageal and pharyngeal injuries associated with the use of the esophageal-tracheal Combitube. Tracheoesophageal fistula caused by cuffed tracheal tube: Successful treatment by tracheal resection and primary repair with four-year follow-up. Delayed diagnosis of esophageal perforation following intraoperative transesophageal echocardiography during valvular replacement: A case report. Time course of esophageal lesions after catheter ablation with cryothermal and radiofrequency ablations: Implication for atrioesophageal fistula formation after catheter ablation for atrial fibrillation. A fatal complication due to radiofrequency ablation for atrial fibrillation: Atrioesophageal fistula. A case of traumatic rupture of the distal esophagus: the importance of early diagnosis. Seatbelt injury causing perforation of the cervical esophagus: A case report and review of the literature. Management of the cervical esophagus and hypopharynx perforations complicating anterior cervical spine surgery. Detection and evaluation of aerodigestive tract injuries caused by cervical and transmediastinal gunshot wounds. Penetrating visceral injuries of the neck: Results of a conservative management policy.
Usefulness of serological IgG antibody determinations for confirming eradication of Helicobacter pylori infection treatment of pneumonia order remeron 15mg fast delivery. Evaluation of four different fecal tests for determination of cure after Helicobacter pylori treatment medications that interact with grapefruit 15mg remeron free shipping. Application of polymerase chain reaction-based assays for rapid identification and antibiotic resistance screening of Helicobacter pylori in gastric biopsies. The most important diagnostic modalities for Helicobacter pylori, now and in the future. Guidelines for the management of Helicobacter pylori infection in Japan: 2009 revised edition. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: A randomized trial. Meta-analysis: Sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Efficacy of 5-day levofloxacin-containing concomitant therapy in eradication of Helicobacter pylori infection. Bismuth-based quadruple therapy using a single capsule of bismuth biskalcitrate, metronidazole, and tetracycline given with omeprazole versus omeprazole, amoxicillin, and clarithromycin for eradication of Helicobacter pylori in duodenal ulcer patients: A prospective, randomized, multicenter, North American trial. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: A randomised, open-label, non-inferiority, phase 3 trial. One-day quadruple therapy compared with 7-day triple therapy for Helicobacter pylori infection. Review article: Rifabutin in the treatment of refractory Helicobacter pylori infection. Risk factors for failure of Helicobacter pylori therapy-Results of an individual data analysis of 2751 patients. Culture-based selection therapy for patients who did not respond to previous treatment for Helicobacter pylori infection. Update on non-bismuth quadruple (concomitant) therapy for eradication of Helicobacter pylori. Pattern of primary resistance of Helicobacter pylori to metronidazole or clarithromycin in the United States. The recurrence of Helicobacter pylori infection: Incidence and variables influencing it. Proton pump inhibitor, clarithromycin and either amoxycillin or nitroimidazole: A meta-analysis of eradication of Helicobacter pylori. Risk of recurrent Helicobacter pylori infection 1 year after initial eradication therapy in 7 Latin American communities. Some define it as a symptom complex, others as an abnormal endoscopic appearance of the stomach, and still others use the term to connote microscopic inflammation of the stomach, usually the mucosa. There is a weak relationship between the presence of histologic gastritis and gastric symptoms (epigastric pain, nausea, vomiting, bleeding). In 1 study of 400 patients, histologic gastritis was present despite a normal gastroscopic examination in 14%, whereas 20% had an abnormal gastroscopic examination with normal histology. By definition, gastric biopsies must be obtained to be able to diagnose gastritis. Indications for gastroscopic biopsies may include gastric symptoms, gastric erosion or ulcer, thick gastric fold(s), gastric polyp(s) or mass(es), and for diagnosis of Hp infection. The location of the biopsy sites should be identified for the pathologist on an accessioning form. Every biopsy represents an excellent opportunity for the clinician and pathologist to communicate to correlate clinical data, endoscopic findings, and pathology. Errors may occur when the pathologist attempts to interpret biopsies without clinical input.
Conventional therapeutic measures medications like lyrica generic remeron 30mg on-line, such as prokinetics symptoms multiple sclerosis discount 15 mg remeron with mastercard, antiemetics, and laxatives, have limited benefit. Hematologic Malignancies the liver, as part of the reticuloendothelial system, is frequently involved in disseminated lymphoproliferative disease and is of significant clinical importance, since it indicates an advanced stage. The frequency of liver involvement varies widely depending upon the type of malignancy. Alternatively, some hepatic abnormalities may be due to drug toxicity, infections, amyloidosis, or extrahepatic obstruction from enlarged porta hepatis lymph nodes. Rarely, massive hepatic infiltration by tumor can result in acute liver failure, with an average survival of 10 days; this syndrome is a contraindication to liver transplantation. This disease presents predominantly with tumor nodules distributed diffusely throughout the liver with a dense lymphomatous infiltrate. The less common T cell lymphoma lacks a typical infiltration pattern and may be confused with a druginduced or viral hepatitis when biopsies just show increased numbers of T cells. A predominantly portal infiltration is the most common histologic feature, with Reed-Sternberg cells detected only occasionally. Treatment reduces proliferation of normal cells, causes myelosuppression, and weakens areas of the bowel wall as it destroys the underlying malignancy. While most patients are asymptomatic, others may complain of abdominal pain, bleeding, or diarrhea. Common oral problems include xerostomia, gingival bleeding, mucositis, infections (particularly candidal), and dental disease. Leukemic infiltrates are found particularly in the terminal ileum and appendix, owing to the abundant lymphoid tissue in these areas. Coagulation defects can produce intramural hematomas and hemorrhagic necrosis of the bowel. Painful anorectal lesions include thrombosed hemorrhoids, stercoral and neutropenic ulcers, fistulas, and abscesses. Other conditions associated with neutropenia may also be complicated by neutropenic enterocolitis. Distension of the cecum, sometimes associated with hypotension, impairs perfusion, leading to mucosal breaches and entry of organisms that proliferate profusely with the neutropenia. Infiltration of liver, spleen, and lymph nodes is common in leukemia, but the possible hemorrhagic complications resulting from liver biopsy make it difficult to discern the relative contributions of leukemic infiltrates, extramedullary hematopoiesis, and other infectious and toxic complications of these diseases. Computed tomography of the abdomen with oral contrast in Axial (A) and coronal (B) reconstructions show severe wall thickening of the cecum with pericecal inflammatory changes (arrows). They include abdominal pain, diarrhea, and nausea/vomiting, often exacerbated by precipitants such as drugs, stress, and certain foods. Occasionally the esophagus is affected with heartburn/ esophagitis or motor disorders. Also, while villous atrophy is found, the crypt hyperplasia typical of celiac sprue is usually not seen. Portal hypertension may develop with esophageal varices, ascites, and splenomegaly, although splenomegaly may also be due to mast cell infiltration. For aggressive disease with organ dysfunction, cytoreductive therapy with interferon or cladribine should be considered. The prognosis is good for the indolent or smoldering type (the latter with organ infiltration without organ dysfunction) but poor for the aggressive type (organ infiltration with dysfunction) or transformation to mast cell leukemia. Histology shows clumps of erythroid and myeloid precursors along with megakaryocytes in the sinusoids, space of Disse, and portal tracts. The most common form is diffuse infiltration, but well-defined nodules or masses, usually multiple, may be seen. Myelofibrosis is characterized by clonal myeloproliferation with bone marrow fibrosis and extramedullary hematopoiesis. Thrombotic complications have been associated with myelofibrosis, polycythemia vera, and essential thrombocytosis. Up to 50% of patients with Budd-Chiari syndrome have an overt myeloproliferative syndrome. Langerhans cell histiocytosis (also called histiocytosis X, eosinophilic granuloma, Letterer-Siwe disease, and Hand-SchullerChristian disease) is an uncommon disorder involving mainly infants and children. Affected patients complain of vomiting, bleeding, diarrhea, constipation, and/or perianal disease. The diverse endoscopic findings include nodules, ulcers, polyps, luminal narrowing, and colitis.