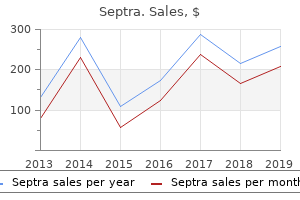
"Buy septra 480mg amex, ombrello glass treatment".
By: U. Tangach, MD
Assistant Professor, University of South Florida College of Medicine
Cheap septra 480mg on-line
False-negative reactions (negative antigen test result symptoms 6 weeks pregnant purchase septra 480 mg overnight delivery, positive culture) may be due to the presence of antigen in the specimen at concentrations below the test detection limit medicine 02 septra 480mg discount. Prozone occurs when the relative concentration of antibody exceeds the concentration of antigen. In this situation, each antigen combines with one or two antibody molecules, and cross-linking between antigen and antibody does not occur. When the concentration of antigen exceeds the relative concentration of antibody, cross-linking between antigen and antibody does not occur, and a proper lattice does not develop. Some test kits for antigen require all negative results be retested with a diluted sample to rule out postzone. False-positive reactions (positive antigen test result, negative culture) are more difficult to explain; they may be due to the presence of cross-reacting antigens or nonviable organisms in the original specimen. Thus an apparent false-positive latex test result may actually represent a true-positive result for disease in a patient with a negative culture. Numerous specimen pretreatment procedures can be used to eliminate or minimize nonspecific agglutinations, presumably by removing or inactivating factors in the specimen responsible for these reactions. These procedures include specimen centrifugation to remove particulate material, boiling to inactivate protein constituents (acceptable when test antigen is a heat-stable polysaccharide), and passing the specimen through a membrane filter. Some specimens, such as urine, may be concentrated by centrifugation or membrane filtration before testing. Filters typically trap or exclude high-molecular-weight antigenic materials, while allowing water and small compounds to pass through. Pretreatments are less frequently required as commercial latex kits become more specific and sensitive. Disadvantages include subjectivity in reading endpoints and nonspecific reactions resulting from interfering substances in clinical samples. In many clinical laboratories, serogroup identification of the -hemolytic Streptococcus spp. Instead of a latex bead, intact formalin-killed Staphylococcus aureus cells (typically Cowan 1 strain) are used. It has been estimated that each staphylococcal cell has about 80,000 antibody-binding sites. The actual number of antibody molecules bound to the staphylococcal cell is limited by stearic hindrance. However, coating is sufficient to render the product of clinical utility in direct antigen tests. Coagglutination procedures appear more susceptible to nonspecific agglutination reactions, and specimen preparation is important. Therefore these reagents are often used to confirm the identification of bacterial colonies on culture plates but not for rapid antigen detection from clinical specimens. The blue color is an indicator dye added to make the agglutination reaction easier to read against a white background. In order for agglutination to occur, antibodies binding to the cells must be sufficiently large to span the cells and overcome the charges. The repulsion of cells by the zeta potential can be affected by pH, low ionic salt solution, and fluid viscosity. In the case of infectious mononucleosis, human heterophile antibody reacts with horse, ox, and sheep erythrocytes. In the appropriate setting, heterophile antibody testing is diagnostically useful and is still used in clinical laboratories. This test takes advantage of the fact that many viral agents, including rubella and influenza viruses, have surface antigens that can agglutinate erythrocytes from certain mammalian species. Antibodies present in sera can bind to the virus and inhibit the agglutination reaction. In addition, the liposome vesicle may be constructed with a chemical dye or bioactive molecule trapped in the interior.
Buy septra 480mg amex
The catalyst medications ending in zole order septra online from canada, usually palladium-coated alumina pellets aquapel glass treatment cheap septra master card, removes residual oxygen from the atmosphere in the chamber. With time, the catalyst pellets become inactivated by water and gaseous metabolic end products produced by the anaerobes, particularly hydrogen sulfide. Silica gel is sometimes used as a desiccant to absorb the water formed when hydrogen combines with free oxygen in the presence of the catalyst and from water vapor from the bacterial media. Unfortunately, the gel can be overwhelmed and become saturated without the users knowing. Desiccants that change color when saturated are not recommended because of the fine powder they contain that can circulate throughout the chamber. Carbon dioxide is required for the growth of many anaerobic organisms, and inert nitrogen gas is used as filler for the remaining percentage of the anaerobic atmosphere. Anaerobic gas is one of the biggest expenditures in operating an anaerobic chamber. Using high-quality anaerobic gas (calibrated or certified) substantially increases the cost. Small amounts of oxygen in these gases can generally be removed by the anaerobic chamber. The College of American Pathologists requires that laboratories performing anaerobic cultures verify daily that anaerobiasis is achieved. This requires the use of an oxygen reduction indicator, which can be methylene blue or resazurin. Methylene blue remains white in the absence of oxygen (reduced) and turns blue in the presence of oxygen; resazurin goes from colorless in the absence of oxygen to pink in the presence of oxygen. These agents can be purchased as strips inside foil pouches and opened inside the chamber or ampules that can be broken to expose the reagent to air just before anaerobic inoculation. A problem with this method is that the agents change color at too high a level of oxygen concentration, which can make it difficult to react in time to maintain the viability of strict anaerobes. Digital oxygen indicators are available that offer faster response times to changes in atmospheric concentrations. For small laboratories, in which the volume of anaerobic cultures may not justify the purchase of anaerobic chambers, alternative systems are available. These jars have been used in clinical laboratories for many years, enabling even small laboratories to perform satisfactory anaerobic bacteriology. Some models accommodate a larger number of plates and microtiter susceptibility trays and anaerobic identification strips or trays. This photograph depicts two of the many different types of anaerobic jars available commercially. Numerous gas-generating systems are available and can be divided into newer systems that are waterless and older systems that require water. When water is added to the GasPak envelope, two gases are generated, carbon dioxide and hydrogen. The two gases have a function similar to that in the anaerobic chamber, with H2 combining with oxygen to form water. Hydrogen is explosive, and if the catalyst is not functioning properly, hydrogen gas will accumulate in the jar. A methylene blue oxidationreduction indicator strip is always added to the jar to verify that an anaerobic atmosphere was achieved. However, it may take several hours for the methylene blue indicator to change from blue to white. If the catalyst performs properly, water vapor will be present on the inside of the jar, and the indicator strip will be white. Failure to achieve anaerobic conditions could be the result of a "poisoned catalyst" or a crack in the jar, lid, or O-ring. A poisoned catalyst results from the gases, particularly H2S, produced by anaerobes.
Diseases
- Hydrocephalus skeletal anomalies
- Muscular dystrophy congenital infantile cataract hypogonadism
- Syringomas
- CDG syndrome
- Crandall syndrome
- Chromosome 2, monosomy 2q24
- Phosphoribosylpyrophosphate synthetase deficiency
- Mucopolysaccharidosis
Discount septra 480mg
Analyzes specimens according to laboratory procedures for the workstation; knows theory and principles of the tests being performed 4 treatment models purchase discount septra. Clearly records all work done so that another person could take over the work station 5 medications going generic in 2016 order septra 480mg otc. Consistently performs and records quality control and documents all remedial action 8. Laboratories are required to maintain successful performance on proficiency testing. Unsuccessful performance is defined as a failure to achieve satisfactory performance for two consecutive or two of three consecutive testing events. If the problem cannot be resolved, an onsite evaluation may be conducted, which may affect accreditation status and force the laboratory to stop testing. Proficiency testing samples are to be assayed in the same manner as patient material, except that no proficiency testing sample shall be referred to another laboratory for analysis. A laboratory is not to test proficiency testing samples on more than one instrument or by multiple methods unless that is how patient specimens are processed. In microbiology, microorganisms in proficiency tests must be identified in the same manner as clinical specimens. Indicators of Performance Improvement: Process Versus Outcome Many types of monitors or indicators can be incorporated into a quality improvement program. This procedure establishes a trend and makes problems easy to detect as disruptions in the trend. Outcome monitors are measurements of the result of a process, such as complications that a patient experiences as the result of a process. Problem-Action Form A simpler approach to monitoring or documenting quality issues is a problem-action form. This approach is most commonly used to document issues that are quickly resolved, but could also be used for long-term monitor summation. The components of the recommendation are to plan, design, measure, assess, and improve. Rather, it should be a coordinated, organization-wide approach for improving patient outcomes that includes interdisciplinary collaborative actions. Internal comparisons or comparisons with similar processes in other organizations are appropriate. Guidelines for assessments might be accreditation standards, practice guidelines, or legal and regulatory requirements. However, specimen collection and processing could have been performed incorrectly. Monitoring of false-negative results for group A streptococci could identify a pattern requiring intervention to improve results. Laboratory professionals may judge quality in terms of accuracy, whereas a physician views it as turnaround time, the patient as compassion and relief from pain, and the insurance company as cost-effectiveness. The patient had to drive from the urgent care facility to the hospital to have the blood drawn by a phlebotomist who was trained in the appropriate techniques No employees at the urgent care facility have been trained to collect blood cultures. This is the second occurrence in about 2 months Seriously ill patients should not have to travel from one facility to another to have their blood drawn. Laboratory administration was informed of this situation All outpatient sites will receive training and written instructions for the proper collection of blood for culture. Patients will no longer have to drive to the hospital for this service if they are already at an outpatient facility M. Benchmarking was initially practiced in business and industry but has now become an important part of hospital quality management programs. A hospital may join a large group of other hospitals that all share operating statistics. Productivity and cost-effectiveness are two large categories commonly used in a benchmarking comparison. A code of conduct is followed when benchmarking is performed that includes ethics and etiquette. Although hospitals generally benchmark other hospitals, they eventually incorporate lessons from other successful industries. Q-probes have covered topics such as adequacy of sputum cultures, turnaround time for spinal fluid Gram-stain results, blood culture contamination rates, and appropriateness of ordering patterns for stool specimens.
Buy 480 mg septra fast delivery
However 5 medications related to the lymphatic system purchase septra without a prescription, assays cannot distinguish an immune response between vaccination or infection medicine tablets trusted septra 480 mg. Detecting antipertussis toxin antibody by enzyme immunoassay or bead-based assays is recommended for diagnosing exposure to B. What factors of Legionella can contribute to the colonization of human-made water supplies What presumptive identification methods are currently used to identify Legionella spp. Besides respiratory tract specimens, what clinical specimen is useful for the sensitive detection of Legionella antigen Which method is preferred for the detection of Bordetella in nasopharyngeal smears Is serology a good method to identify and respond to pertussis outbreaks in real time Erythromycin is important for eradication of the organism and prevention of secondary cases but has clinical efficacy only if treatment is started during the catarrhal phase of disease. Azithromycin has fewer and milder side effects, has a longer half-life, and requires fewer daily doses resulting in better patient compliance. Trimethoprim-sulfamethoxazole is also an alternative for treatment or prophylaxis. Sources include contaminated potable water distribution systems, respiratory therapy equipment, and recreational waters. Pontiac fever is a milder febrile disease resembling influenza that may be caused by inhalation of bacterial toxin. The central portion of young colonies have a "ground glass" appearance, light gray and granular, whereas the periphery of the colony has pink or light blue or bottle-green bands. Acid treatment of specimens contaminated with other bacteria before inoculation enhances isolation of Legionella spp. Nasopharyngeal aspirates or swab specimens should be plated directly onto culture media or transferred to an appropriate transport system (casamino acid or Amies transport medium) at the bedside. Establishment of diagnostic cutoff points for levels of serum antibodies to pertussis toxin, filamentous hemagglutinin, and fimbriae in adolescents and adults in the United States. Surveillance for travel-associated legionnaires disease-United States, 2005-2006. Outbreaks of respiratory illnesses mistakenly attributed to pertussis-New Hampshire, Massachusetts, and Tennessee, 2004-6. Recommended immunization schedule for children and adolescents aged 18 years or younger, United States, 2017. Surveillance of vaccination coverage among adult populations-United States, 2014. Infectious Diseases Society of America/ American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Current and emerging Legionella diagnostics for laboratory and outbreak investigations. List the general characteristics of organisms that belong to the family Enterobacteriaceae. Describe the antigenic structures of the family Enterobacteriaceae, and explain how these antigens are used for identification. Compare the virulence factors of the Escherichia coli strains pathogenic for the gastrointestinal tract and the E. Compare the pathogenesis of the three species of Yersinia most often recovered from humans. Describe the pathogenesis of the clinically relevant members of the family Enterobacteriaceae.
Buy discount septra line
They hydrolyze esculin and are indole positive treatment yeast infection nipples breastfeeding discount septra generic, and growth on MacConkey is variable symptoms uterine prolapse septra 480mg mastercard. Itwasfirst isolated in 1987 during an outbreak of pneumonia and meningitis linked to individuals attending a hot springs spa. The organism is saccharolytic, oxidizing glucose, mannose, fructose, and other sugars. Ubiquitous in soil and water, they are rarely isolated from clinical specimens but have been found in hospital equipment and fluids. Isolates of Comamonas testosteroni and Comamonas terrigena have been reported to cause nosocomial bacteremia. Delftia acidovorans has been associated with keratitis in soft contact lens wearers and nosocomial infections including bacteremia and endocarditis. Isolated cases of endophthalmitis have been reported to be caused by Empedobacter brevis following cataract surgery. Members of the genus Wautersiella have been isolated from blood and surgical wounds. Members of the genus Sphingobacterium at one time were regarded as members of the genus Flavobacterium. Onmediawithblood,a lavender-green discoloration of the agar may occur because of the proteolytic activity of the organisms. All except Myroides and Sphingobacterium are indole positive, a distinctive characteristic among this family. In vitro, most species are resistant to aminoglycosides and -lactam antibiotics, but some species are susceptible to vancomycin, which is an unusual characteristic for gram-negative bacilli. However, one report of susceptibility testing of more than 50 isolates of Chryseobacterium spp. Methylobacterium and Roseomonas the genus Methylobacterium contains 20 named species plus additional unnamed biovars; isolates produce a characteristic pink to coral pigment and can use methanol as a sole source of carbon andenergy. Epidemiologically,theMethylobacterium are isolated from soil, vegetation, sewage, water, and hospital nebulizers. They have also been recovered from clinical specimens such as throat swabs, bronchial washes, and even blood specimens. Clinically, these organisms have been reported to cause bacteremia, peritonitis, synovitis, and skin ulcers, usually in immunocompromised hosts. Contaminated tap water has been implicated as a cause of positive blood cultures in a patient receiving irrigations who had recently undergone bone marrow transplant; a leukemic patient who had undergone stem cell transplant was found to have bacteremia with Methylobacterium fujisawaense. They are variable in the oxidase reaction, often weak to negative, but isolates are catalase and urease positive. Although uncommon isolates, they are the most common pink-pigmented, gram-negative, nonfermentative bacillus recovered in clinical laboratories. Note the growth with yellow pigment on sheep blood agar (left) and absence of growth on MacConkey agar plate (right). Environmental sources, such as stagnant water, natural gas (petroleum), brine, and spoiled dairy products, may contain S. These organisms are usually susceptible to ampicillin, tetracycline, chloramphenicol, erythromycin, and the aminoglycosides, but resistant to penicillin and cefazolin. Isolates can be found contaminating sterile hospital fluids and, as such, may be isolated from specimens including urine, nasopharynx, abscess, wound, and blood specimens, usually as colonizers or contaminants. The unusual practice of moistening culturette swabs with tap water before the collection of microbiology samples led to an outbreak of C. They Sphingomonas Sphingomonas paucimobilis can be isolated from many water sources,includingswimmingpools,aswellasfromhospitalequipment and laboratory supplies. The genus Sphingomonas contains at least 12 species, but only two are believed to be clinically significant:S. Theyaresusceptible to polymyxin B, which differentiates isolates from members of the genus Sphingobacterium, which they resemble. Pseudomonas oryzihabitans cutaneous ulceration from Octopus vulgaris bite: a case report and review of the literature.
Order septra 480 mg free shipping
Interestingly treatment rheumatoid arthritis cheap 480 mg septra otc, recent work has separated out how praxis occurs in the first place into two interconnected mechanisms5: 1 treatment thesaurus purchase septra 480 mg on line. Mechanical knowledge: this is a collection of observations about shapes of objects, physical properties of objects, and mechanical angles. For example, experience teaches one that a flat bladed firm device can fit into a screw head, and turn the screw. This is how we can figure out that a substitute device of similar properties might work for the issue, and how we discard using a piece of paper or a toothbrush for the same task, as they lack the right shape, and strength to do the job. Functional knowledge: this is a collection of facts about tools and actions and how they work. For example, most of us can verbalize that a screwdriver is used to drive a screw, or how to perform a military salute, even if we are not in the presence of this device. Interestingly, problems with mechanical knowledge and functional knowledge can double dissociate. One example are patients who cannot describe what a tool does, or pantomime its use, but who are able to use the tool when it is actually there (because they have mechanical knowledge to navigate the task). The final common pathway for praxis related activity is the motor network, especially the hand motor areas. In most cases, saving speech means saving praxis as the networks are so tightly linked. Note that poor cooperation with mapping tasks can be due to aphasia or apraxia, and this should be considered during surgery. Praxis is more prominently parietal, and should be tested in these regions even if speech mapping is negative, as the cortical sites may not entirely overlap, and the findings can be subtle. In fact, when thinking what to name this network, I decided to keep it just neglect, as it is not purely a spatiotemporal problem, though those issues are certainly involved, and it is not purely an attentional problem, though obviously attention is involved with the problem. First, it is not extinction, meaning an inattention to contralateral stimuli when presented with an ipsilesional stimulus. Extinction runs with neglect in big lesions, but the two have been found to double dissociate, as extinction is a superior parietal lobule problem. It also probably is not synonymous with deviation on line bisection tests, which also double dissociates with neglect, and localizes more posteriorly into visual processing areas and the angular gyrus, probably causing people to see the left side of the line as shorter than the right. The frequent co-existence of these syndromes with neglect is likely due to the physical proximity of these areas which often lie within the same vascular territory. True neglect is a hemispatial inattention syndrome manifested in motor and/or sensory forms. One form is termed egocentric neglect (alternately called spatial centered neglect), which is the form we typically associate with neglect. These patients ignore objects in their left hemispace, fail to read words on the left side of a page etc. This subtype of patient does not neglect the entire left side in pure form, but rather neglects the left side of objects. Interestingly, these patients will neglect the left side of an object even if it is placed within the right visual field, strongly suggesting that there is a dual pathway which processes spatiotemporal awareness both from an egocentric perspective on a coordinate system relative to the individual, and an allocentric perspective where individual objects are analyzed as whole entities and the coordinate system is relative to the object. Further, previous articles on neglect have demonstrated that recovery from stroke induced neglect depends on the degree of white matter injury of the periventricular white matter, strongly tying neglect into a white matter network disease. The problem with viewing this as such is that unlike language, which is substantially lateralized such that a unilateral injury involving both sides (aphasics cannot talk using the left side of their mouth), unilateral injury to the right side only causes left neglect as opposed to neglecting both sides. This strongly argues that the network is bilateral to some extent, but that the right side is dominant and that the left cannot compensate for it if it goes down. Clearly the easiest thing is to term this network as the spatiotemporal network, as it is likely results in part from the failure to transmit information about coordinates about 3D space on an egocentric and/or allocentric grid. But the presence of neglect in some patients with thalamic or medial frontal injuries calls into question that there is not an attentional component. I think in the absence of more information about the exact anatomy of this problem, our best way to view this is that this part of the parietotemporal junction involves a transformation from the complex multimodal and comparative signal of association cortices, which provide various types of processing of visual input (including directionality, motion, rotation specific neurons among others), auditory input, somatosensory, cerebellar, proprioceptive (eye, head, neck and arm position data needed to create a grid), converting this information to simpler outputs needed to interact effectively with the motor system. The Key Players the Supramarginal Gyrus this is not consistent; however, it is likely part of the network, especially of egocentric representations of 3D space. Superior Temporal/Middle Temporal Gyrus these gyri are classically part of the semantic network, which probably performs an analogous transformation to the left side, only with object recognition being transformed into coordinates centered on that object, instead of creating a name as with the left side.
Hydrolyzed Chicken Collagen Type II (Chicken Collagen). Septra.
- How does Chicken Collagen work?
- Dosing considerations for Chicken Collagen.
- Are there safety concerns?
- Pain associated with many types of arthritis, post-surgical joint pain, post-traumatic pain, and back and neck pain.
- What is Chicken Collagen?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96699
480mg septra free shipping
Thus treatment statistics buy 480mg septra overnight delivery, I resect the insula until the lateral aspect of the resection cavity is roughly parallel with the hippocampus in the sagittal plane symptoms pancreatitis purchase septra master card. Obviously, this is a judgment call, and you should also be continually looking for tissue characteristics suggesting that you are in the putamen (putamen tissue looks like the caudate head tissue grossly), as it can look deceptively like tumor and you can remove a fair bit of putamen before you realize you are in it. Not only does it indicate the approximate depth of the basal ganglia, but it also prevents you from entering the basal ganglia from below when it is present. Medial-to-lateral orientation is easy to lose when there is nothing preventing you from working on the undersurface of the central cerebral core, and it is easy to drift into the wrong plane, and into trouble. The presence of the hippocampus prevents this from occurring, and serves as a depth gauge. If you have approached solely from the frontal side, you lack this depth gauge and it is harder to tell how deep to go. Obviously, subcortical monitoring is one source of this information, and the appearance of putamen tissue is another, but also the angle of access to the insula in the frontal transopercular approach parallels the cortex, meaning heading too medial is not usually a natural maneuver (usually you have to force yourself medial or you will be inadequately resecting tumor. It is easy to become disoriented in the insula, and as soon as you start removing tumor, you begin to destroy the anatomy, making it very hard to re-orient yourself. This is a logical extension of subsequent rules, but remember that it is a lot easier for parts of the insula to hide behind arterial complexes than you think. This will be unnerving the first time you do it, but this is what resecting the insula means. You must discipline yourself to not do so, and to follow rule 2, even if that means working in a less comfortable window. You have to manipulate the arteries and gently retract them in order to do this case, but if you get too greedy with a window, you can tear a main trunk at its branch point, which is dangerous and unpleasant. If you are working far under an artery, even if you think you can keep going, you should explore other windows and work towards using all of your spaces instead. Bifurcations are great places to overstretch arteries, as often one branch is often leaving the fissure and is tethered to the operculum. You will often have to work inside a tight bifurcation, but you should strongly consider only doing so long enough to detach the brain immediately in the "V" of this bifurcation, and then use this new mobility to work on both sides of the "V" which is usually roomier. A temporal lobectomy was performed as part of a transopercular resection of the insula. The lateral part of the anterior temporal lobe has been removed but the insula is quite large, the hippocampus is full of tumor, and the tumor extends into the premotor areas. This will seem overly aggressive if you have never done this before, but it is well tolerated if other anatomy is respected. Of note, we utilized the previous incision, which was larger than I would normally do. I decided not to (it was earlier in my series; today I probably would try under the idea that it may be difficult). Spatiotemporal mapping limited the posterior cut, slightly but despite this, this was a complete resection. The obvious approach in a case like this is to approach this from the temporal lobe side as a lobectomy is warranted. The sagittal and coronal images show a C-shape of this tumor which is following the uncinate into the orbitofrontal cortex. This should usually be followed upward and anterior into the frontal lobe through the insula. Note that with continuous subcortical monitoring, we took this resection right up to the internal without deficit. I have seen this at least 15 times in various insular gliomas and have never seen this area progress without treatment once, even when followed for a few years. I suspect that this is some kind of Wallerian degeneration involving some aspect of the posterior thalamic peduncle as I have followed the signal change on multiple cuts in these cases and have never seen one which directly connects the insula and pulvinar with signal change and have never seen one of these combos cross the internal capsule to get there. It could always be spread on a microscopic level, I acknowledge; however, until I see one progress in the thalamus, I will continue to leave the thalamic part alone in these cases.
Purchase septra in india
Note that this is easy to do medicine quotes buy discount septra 480 mg on line, as you are working down the long axis of the temporal lobe at the depths of an occipital lobectomy; however 4 medications at target buy septra 480 mg lowest price, caution is advised as it is easy to become disoriented from this angle. Disorientation from this angle usually takes you into the internal capsule or central core. The bed is rotated when we remove the medial temporal portions so that the lip of brain along the lateral cut does not fall into our way. Note that once you locate the atrium and the edge of the tentorium, you can follow the medial temporal structures as far anteriorly as you wish provided you stay below and medial to the temporal horn. The deep part of this tumor abuts the optic radiations, and this tumor is clearly in visual processing areas. You can discuss at length whether a marginal resection or a lesionectomy is better for this case: I performed a compromise between lobectomy and lesionectomy. This is obviously a very difficult decision, as we would wish to save the ipsilateral visual system if possible, in patients where it is functioning. A few arguments for aggressive resection based on anatomic boundaries: 1) the depth of this tumor is close to the optic radiations, making them hard to save and still remove the tumor, 2) as the maps in Chapter 6 demonstrate that visual processing is a series of sites which process in sequential fashion and are connected via numerous small local connections and interconnections. They are also interconnected with the thalamus at multiple steps, and I feel that it is likely that cutting anywhere along the chain (especially early stages such as V2 or V3) would eliminate visual output in the same way as resecting V1. Again, those willing to sacrifice tumor control for function often end up with neither, and we should always be aware of this in our tradeoffs. This patient had an early recurrence, and at recurrence the tumor not only regrew in the surgical cavity, but also followed the connections with this area to the pulvinar, which is predictable based on the connectivity of this region. The answers are never as clear in prospect as in retrospect, but in hindsight, I view this as a poorly thought out tradeoff on my part between function and tumor control that ultimately achieved neither for long. But a closer look shows that this tumor is following the lateral occipital pathways into the deep white matter, and thus puts numerous pathways at risk. I spent several hours in this case patiently teasing this tumor away from the deep white matter. Anatomic resection was not realistic here, so we based the resection on gross appearance and functional information. I settled for the resection seen in these images, and was very happy I got out as much as I was able to without any speech problems. They are case examples and the files are organized as follows: (a) preoperative images, (b) intraoperative image. These tumors provide the challenging feature of extending below the sensorimotor cortex by following in the cingulate gyrus. The technique for removing them is similar to a medial parietal case (they often are in these parts of the parietal lobes given the interconnection with the cingulum and superior parietal lobule). After providing access to the posterior cingulate, I determine what aspects of the posterior cingulate can be removed, with concentration tasks, usually I find that it has reorganized and can be taken in most cingulate tumors. It is then critical to define the cingulate sulcus and stay between it and the callosum as you remove the cingulate under the sensory and motor strip. When you first see one of these uncommon tumors, you generally will mistake it for a medial parietal tumor. In insular tumors, this is an opercular resection, but in this case it is a medial parietal resection. Once this is complete, you have excellent access to the boundaries of the deeper structure, and can see what you are doing. You can get lost in the cingulate just like the insula and you need to identify and remain in the safe boundary landmarks. This can be appreciated on all sequences, but especially on the sagittal, where the motor fibers create a tunnel where the cingulate tumor must pass through. The callosal fibers are colored in purple as well, and these also form a tunnel for the cingulate. While there are still T2 changes in the motor system, overall this is a good resection. Note that there are distinct aspects of this resection cavity which reflect a medial parietal resection followed by cingulate removal. These are tumors which are obviously high risk, and ones which many, often good tumor surgeons deem "inoperable.
Discount 480mg septra fast delivery
Which of the following refers to the ability of a test to detect a particular analyte If 100 individuals without syphilis were tested for the disease and 95 tested negative medications prolonged qt order genuine septra on line, what is the diagnostic specificity of the test What parameter would be used to determine the percentage of patients who are appropriately classified as having a disease or not having a disease Clinical Laboratory Improvement Act of 1988: Rules and regulations medications for migraines buy discount septra 480 mg online, Fed Reg Feb 28, 1992. Performance standards for antimicrobial disk susceptibility tests: approved standard, ed 10 (M02-A10). State the goal of specimen preservation, storage, and transport to the laboratory. Select the appropriate conditions for storage of specific specimen examples, such as urine and fecal samples. Explain the prioritization guidelines used during processing to prevent degradation of the specimen. Analyze situations in which specimens are unacceptable, and summarize the action to be taken. List the characteristics that can be noted from a macroscopic observation of the specimen. Summarize the purposes of a direct microscopic examination, and identify specimen sources where this technique is utilized and specimens where the technique is not beneficial and not performed. Compare the categories of media used in clinical microbiology, and explain how media are selected. Determine the appropriate isolation technique to be used for each specimen source when inoculating solid media. Specify the appropriate temperature and atmospheric conditions for incubation of routine specimens and to recover fastidious bacteria. Assess the significance of the communication of microbiology findings and the role of the laboratory in the postanalytic process. The microbiology technologist began to streak through the area of inoculation on the plate and noted that the medium appeared dry. The microbiology technologist must recognize and reject suboptimal specimens and educate other members of the medical team. Aspiratedmaterial should be placed into a sterile tube or transport vial and not "squirted" onto a swab. Patient-Collected Specimens In certain situations, patients are asked to collect the specimen themselves. The instructions should be written in simple language and pictures to help the patient understand the procedure as it is verbally explained. A first morning specimen is preferred because it provides a more concentrated sample. The patient collects this specimen following cleansing of the external genitalia to reduce the presence of indigenousflora. Forthisreason,theyareone of the least clinically relevant specimens received for culture. The patient needs to understand the difference between sputum, saliva, and nasal secretions. Patients should rinse their mouth with water and expectorate with the aid of a deep cough directly into a sterile container (expectorated sputum). Iffungal or mycobacterial infections are suspected, three separate early morning specimens are appropriate. Respiratory therapy technicians may assist patients who are unable to expectorate a respiratory specimen. Stool the specimen of choice for the detection of gastrointestinal pathogensisstool. Inaddition,thepatient needs to be told that the specimen must be thoroughly mixed withthepreservative. All that the laboratory knows about the patient is learned from the requisitionform. Leaking containers and specimens with needles attached present the greatest hazards.
Buy septra 480mg without a prescription
Most assays designed to detect IgM antibody include some initial procedure to separate IgG physically from IgM or to "capture" IgM in the assay and then remove IgG symptoms indigestion septra 480 mg without a prescription. A false-positive serologic test result is a positive result for a patient who is not infected by the specific agent for which the test is designed medicine of the prophet buy septra online pills. It might occur from the production of cross-reacting antibody, as discussed previously, or from the reactivation of a latent organism as a result of infection by a different organism. Finally, individuals receiving intravenous immunoglobulin, a product prepared by pooling large quantities of plasma from multiple volunteer donors, may show specific antibody to various infectious agents because of passive transfer, not active infection. Laboratory personnel must be aware of this possibility and any therapy that may be of significance in interpreting serologic test results for a specific patient specimen. Population Studies Serologic tests for a specific infectious agent or a battery of agents may be performed to determine the percentage of individuals previously exposed or infected with the agents in a geographic area. This information provides epidemiologists and public health officials with information about how widespread an infectious agent is in a given area. Such studies have shown that the fungus Histoplasma capsulatum, which causes histoplasmosis, is widely distributed in the Ohio River Valley and that the bacterium Borrelia burgdorferi, which causes Lyme disease, is common in the Upper Midwest, New England, and Middle Atlantic states. Similarly, serologic studies performed on animals that are reservoirs for human disease may alert public health officials that a disease. Excess antigen-specific immunoglobulin G (IgG) inhibits antigen-specific IgM from binding. Immune Status Testing In several situations, it may be important to determine whether an individual is immune (through either previous infection or immunization) to a specific infectious disease. This requirement exists because if employees are infected, they can transmit the virus during the incubation period (before symptoms develop) to susceptible patients. Infection with varicella-zoster virus in a newborn or immunosuppressed patient may be life-threatening. It is generally recommended that all women of childbearing age be tested for their rubella immune status; if it is negative, they should be vaccinated before considering pregnancy. An additional situation in which immune status testing might be considered is organ or bone marrow transplantation. Congenital Infections Serologic testing is often used to help diagnose congenital infections (acquired in utero) in a newborn; some infectious agents have the ability to cross the placenta and cause infection of the fetus. Such infections might cause only minimal symptoms in the mother during pregnancy and may go undiagnosed at the time. However, if the mother is nonimmune, the infection can be significant to the fetus. Similarly, testing for IgG antibody in the newborn is of no value because maternal IgG crosses the placenta and is present in neonatal serum. Testing for maternal IgM antibody is likewise of little value (unless infection occurred near the time of delivery), because it may be undetectable by 1 or 2 months after infection. These antigens can be recognized by and combine specifically with antibody molecules to form stable complexes. The basic process of antigen detection involves mixing a clinical specimen with an antibody preparation specific for the antigen of interest. If the microbial antigen is present in the specimen, an antigen-antibody interaction occurs, forming an immune complex. Many techniques use indicator molecules such as enzymes and substrate, fluorochrome excitation, or chemiluminescence. The tests used to detect these proteins (antigens) are similar to tests used in the detection of antibody. Principles of Immunologic Assays Precipitation Assays the precipitation reaction is found in assays involving the diffusion of soluble antigen and antibody. At a critical point, when the concentrations are optimal, a visible precipitate forms, which is composed of an insoluble complex of antigens and antibodies. Precipitation methods with diagnostic significance for infectious diseases are double immunodiffusion, radial immunodiffusion, and flocculation tests. The antigen and antibody molecules in solution diffuse out of the wells and through the porous agarose. If antibody specific for the antigen is present, the two components combine at a point of optimal concentration Antigen Detection Antibody detection can require a significant length of time to become positive.
References: