"Buy discount zithromax 100 mg on line, virus ti snow".
By: W. Dennis, M.A.S., M.D.
Assistant Professor, State University of New York Downstate Medical Center College of Medicine
Generic zithromax 100mg mastercard
Angiogenesis is the process of formation of new blood vessels from existing vessels antimicrobial humidifier discount 500 mg zithromax otc. The term granulation tissue is derived from its pink treatment for dogs diarrhea purchase generic zithromax line, soft, granular appearance on the surface of healing wounds. Healing by Primary Union or by First Intention Definition: Healing of a clean, uninfected surgical incision in the skin joined with surgical sutures is known as healing by primary union or by first intention. Surgical incision causes death of a minimum number of epithelial and connective tissue cells. Blood clot contains not only trapped red cells but also fibrin, fibronectin and complement components. Dehydration at the external surface of the clot leads to formation of a scab over the wound. Neutrophil infiltration: Within 24 hours of wound, neutrophils appear at the margins of the incision. Epithelial changes: At the cut edges of the wound, the basal cells of the epidermis begin to show mitotic activity. Epithelial cells from both the edges of wound proliferate and migrate across the wound along the dermis. The epithelial cells fuse in the midline below the surface scab and epithelial continuity is re-established in the form of a thin continuous surface layer. Collagen deposition along the line of stress and wound gradually achieves maximal 80% of tensile strength of normal skin. Definition: When injury produces large defects on the skin surface with extensive loss of cells and tissue, the healing process is more complicated. Healing in such cutaneous wound is referred to as healing by secondary union or by second intention. Myofibroblasts of granulation tissue have ultrastructural features of smooth muscle cells. Feature Nature of wound Margins Sutures Infection Amount of granulation tissue Outcome Complications v Primary intention Clean surgical wound Surgical clean margin Used for apposition of margins Absent Scanty at the incised gap and along suture track Neat linear scar Rare Secondary intention Unclean Irregular Cannot be used May be infected Abundant and fill the gap Irregular contracted scar Infection and suppuration At the end of the first week: When sutures are removed from an incisional surgical wound, wound strength is about 10% that of normal unwounded skin. Four weeks: Wound strength quickly increases over the next 4 weeks, and then slows down. Differences between healing by primary and secondary intention is discussed in Table 3. Compare/tabulate the differences between wound healing by primary and secondary intention with suitable diagrams. Basic mechanisms of healing by primary (first intention) and secondary (second intention) union are similar. Wound contraction is an important feature of healing by secondary intention and is mediated by myofibroblasts. Mechanical factors: Movement of wounded area may compress the blood vessels and separate the edges of the wound and can result in delayed healing. Foreign bodies: Unnecessary sutures or foreign bodies (fragments of steel, glass), or even bone can delay healing. Location of injury: Wound over the skin covering bone with little intervening tissue prevents wound contraction. Blood supply: n Varicose veins of the legs decrease the venous drainage and can cause nonhealing ulceration. Size and type of wound: Small surgical incisional or other injuries heal quickly with less scar formation. Blood supply: Wounds in areas with good blood supply, such as the face, heal faster than those with poor blood supply, such as the foot. Nutritional deficiencies: Delays wound healing and these include: n Protein deficiency. Metabolic status: Diabetes mellitus is associated with delayed healing due to microangiopathy. Circulatory status: Inadequate blood supply (due to arteriosclerosis) or venous abnormalities. Hormones: Glucocorticoids have anti-inflammatory effects and also inhibit collagen synthesis, thereby impair wound healing. Hematological abnormalities: Quantitative or qualitative defects in neutrophils and bleeding disorders may slow the healing process.
Buy discount zithromax 100 mg on line
It can produce epilepsy (convulsions) antibiotics for sinus infection and ear infection order zithromax 100mg otc, hydrocephalus ear infection 1 year old buy zithromax with paypal, increased intracranial pressure, blurred vision and other neurologic disturbances. Life cycle: Echinococcus granulosus requires two mammalian hosts to complete its life cycle. The adult worm in small intestines of dogs, discharges eggs in feces which are ingested by man, sheep, pigs and other mammals. The eggs hatch in the human duodenum and are carried to the liver by portal venous system and other sites through systemic circulation. Pericyst (outer, capsular layer): It shows inflammatory reaction and consists of fibroblasts, giant cells, and mononuclear and eosinophils. Ectocyst(intermediate opaque, non-nucleated layer): It is distinctive and has innumerable delicate laminations. Endocyst (inner, nucleated, germinative layer with daughter cysts and scolices projecting into the lumen): Daughter cysts can develop within the large mother cyst. They appear first as minute projections of the germinative layer that develop central vesicles and thus form tiny brood capsules. Degenerating scolices of the worm produce a fine, grain-like (sand-like) sediment within the hydatid fluid (hydatid sand). Cerebral: Epilepsy Renal: Hematuria v Rupture of cyst: the liberation of antigenic proteins in the hydatid fluid into the circulation produces eosinophilia and may even cause anaphylactic reactions. During the mosquito bite to humans, the infective larvae are released by mosquitoes into the tissues. They develop within lymphatic channels into adult males and females which mate and release microfilariae into the bloodstream. During the mosquito bite of the infected persons, the mosquitoes can take up the microfilariae. These microfilariae undergo further development in the mosquito and they become infective and transmit the disease to humans. Adult filarial worms (live, dead, or calcified) are observed in the draining lymphatics or nodes. Usually, it occurs in nasopharynx as polyp but may also be observed in larynx and conjunctiva. On rupture of a sporangium, the spores may be discharged into the submucosa or on to the surface of the mucosa. Individual lesions are small, firm, smooth, often pruritic, pink to skincolored, dome-shaped papules, generally ranging in diameter from 2 mm to 4 mm. Fully developed lesions have a characteristic central umbilication and in a fully-developed lesion, small amount of cheesy (curd/paste-like) keratinous material can be expressed on pressing from the central umbilication. This material if smeared onto a glass slide and stained with Giemsa may shows diagnostic molluscum bodies. The viral inclusions are diagnostically specific structures (which appear ellipsoid) and are termed as molluscum bodies. The viral inclusions are found in cells of the stratum granulosum and the stratum corneum. Under hematoxylin and eosin stain, these inclusions appear faintly granular eosinophilic in the bluepurple stratum granulosum and pale blue in the red stratum corneum. Definition: Hyperemia is an active process in which arteriolar dilation leads to increased blood flow to a tissue/organ. Pathological: Seen in inflammation and is responsible for the two cardinal signs of inflammation namely heat (calor) and redness (rubor/erythema). Definition: Congestion is a passive process resulting from reduced venous outflow of blood from a tissue/organ. Local: Examples include: n Congestion of leg veins due to deep venous thrombosis edema of the lower extremity. Chronic passive congestion: It usually produces edema in the organ/tissue in which the venous outflow is reduced. Write short note on heart failure cells and the special stain used for its demonstration. Pulmonary edema: It is due to forced movement of fluid from congested vessels into the alveolar spaces. Fibrosis: It develops due to increased fibrous tissue in the interstitium of lung. Pulmonary hypertension: It is due to transmission of pressure from the alveolar capillaries to the pulmonary arterial system.
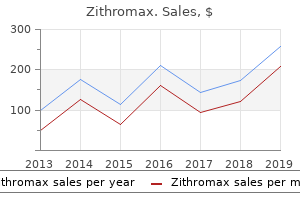
| Comparative prices of Zithromax |
| # | Retailer | Average price |
| 1 | SonyStyle | 600 |
| 2 | Stater Bros. Holdings | 665 |
| 3 | Winn-Dixie Stores | 207 |
| 4 | Albertsons | 256 |
| 5 | Aldi | 655 |
| 6 | Darden Restaurants | 709 |
Buy 250mg zithromax
Slide or Tile Techniques Place one drop of anti-Rh (D) reagent (should be monoclonal IgM type) on a slide/white tile popular antibiotics for sinus infection cheap zithromax american express. Interpretation: Presence of agglutination indicates that the blood sample is Rh +ve virus free 250 mg zithromax mastercard. In test tube method procedure is similar to slide method except that it is performed in a test tube. Microplate Method Microplate method is ideal for testing large number of blood samples and has replaced test tube method in many laboratories. Blood grouping is important before blood transfusion, for pregnant women (for Rh incompatibility between Rh+ ve and Rh-ve mother) and is also of medicolegal value. Other blood group systems: these are weak antigens and have no clinical significance. Blood Transfusion Blood transfusion is the process of transferring blood/blood products from donor into the circulating system of recipient. It is important to properly collect the blood from donor, prepare its components (if required) and store blood/components in a proper way and transfuse in such a way to avoid any risks or hazards. Donor selection is based on medical history and few routine physical examinations (weight, blood pressure, temperature, hemoglobin) are done to know whether donor is suitable for donating blood. There are three types of donors namely voluntary (should be encouraged), replacement and professional. Collection of Blood Blood is collected under aseptic conditions using sterile, plastic bag with anticoagulant. Write short answer on screening of blood unit before transfusion (pretransfusion tests). This is achieved by performing a set of procedures known pretransfusion testing also referred to as compatibility testing. These set of procedures (serologic and nonserologic protocols) are required before blood is sued as being compatible. A compatibility testing is an entire quality process composed of many procedures (steps). It is designed to provide the safest blood product possible for the recipient of the transfusion. Sometimes, the term compatibility test and cross-matching are used interchangeably, but crossmatch is only a part of compatibility test. In crossmatching, the serum or plasma from the recipient is mixed with red cells from the donor. A crossmatch is only one part of pretransfusion (compatibility) testing and is very important before any blood transfusion. Crossmatching is routinely done only with donor products containing red cells, hence must be performed for red cell transfusions. Hemolysis or agglutination at any phase or step of the crossmatch process indicates that the antibodies present in the recipient interact with donor red cell antigens and a mismatch between donor and recipient. A crossmatch is considered as compatible when there is neither agglutination nor hemolysis in testing and the donor unit is acceptable for transfusion purposes. A cross-match is considered as incompatible when there is presence of either agglutination or hemolysis. Types Crossmatching procedure may be divided into two major parts, namely, (i) major and (ii) minor crossmatching (Table 15. Principles of Serological Testing the pretransfusion testing is performed to detect in vitro red cell antigen and antibody reaction by observing for either agglutination or hemolysis. In this method, there should not be any delay in the centrifugation step or reading the reaction. Cells usually are washed once to remove any anticoagulant or plasma protein which may interfere with the testing. Gently dislodge the cell button and examine the tube for the presence or absence of hemolysis or agglutination. Interpretation: v Positive test: If hemolysis or agglutination is present at this stage, the test is considered as reactive/positive. It is always necessary to monitor the recipient during and after transfusion so that any complications can be dealt accordingly.
Buy 100 mg zithromax otc
Evidence of the earliest signs of heart failure bacteria 10 cheap 500mg zithromax mastercard, placentomegaly antibiotic resistance assay order zithromax 500 mg fast delivery, and/or hydrops should be sought, as these may progress rapidly and are harbingers of preterminal events. This approach may be useful in managing the common association of prematurity, large tumor, and hyperdynamic state [44]. Previous results in this setting with radiofrequency ablation have been uniformly poor, however interstitial laser photocoagulation of feeding vessels has been reported to correct the high-output state without the adverse results seen with radiofrequency ablation [49, 50]. Postnatal Management/Outcome A neonatologist should attend the delivery and be prepared to provide respiratory support. Excellent venous access is paramount, along with echocardiography and abdominal ultrasound should hemorrhage in the tumor occur. If there is no high-output state tumor resection is not mandatory and attention should focus on treating respiratory distress and correction of anemia. When the patient is stable, surgical resection consists of excision of both the tumor and the coccyx, which is thought to be essential to prevent recurrence. Congenital cervical immature teratoma arising in the left lobe of the thyroid gland. Approach for oxygenation of the newborn with airway obstruction due to a cervical mass. Management of giant cervical teratoma with intracranial extension diagnosed in utero. Cervical and oral teratoma in the fetus: a systematic review of etiology, pathology, diagnosis, treatment and prognosis. Diagnosis and management of fetal cardiac tumors: a multicenter experience and review of published reports. Rhabdomyoma and ventricular preexcitation syndrome: a report of two cases and review of literature. Successful ultrasoundguided laser treatment of fetal hydrops caused by pulmonary sequestration. Percutaneous laser ablation under ultrasound guidance for fetal hyperechogenic microcystic lung lesions with hydrops: a single center cohort and literature review. Contribution of magnetic resonance imaging to prenatal differential diagnosis of renal tumors: report of two cases and review of the literature. Reference values of fetal aortic flow velocity waveforms and associated intra-observer reliability in normal pregnancies. Preoperative angiography with embolization and radiofrequency ablation as novel adjuncts to safe surgical resection of a large, vascular sacrococcygeal teratoma. Survival rates are higher in tertiary care centers with a minimum case load of more than 10 patients per year and standardized management protocols [11]. Significant advances in postnatal management, such as the introduction of gentle ventilation and permissive hypercarbia, have resulted in improved survival rates over the past two decades [14]. At 28 days of life, half of the survivors are oxygen dependent [16], whereas at discharge 16% still require oxygen [17]. More than 40% of patients need bronchodilators within the first year of life [17], and over 10% suffer from asthma and obstructive lung disease during childhood [18]. In some, chronic lung disease is further exacerbated by abnormal diaphragmatic compliance and thoracic deformities [19]. The causes are multiple and include displacement of the stomach, modification of the gastroesophageal junction and abnormal motility of the esophagus, and some of these changes are induced by the surgery. In addition, malrotation may delay gastric emptying, and the abnormal balance of pressures in the thorax and abdomen facilitates retrograde passage of gastric content to the esophagus [24]. During embryogenesis the diaphragm fails to form [1], most often on the left side (85%), rarely on the right (13%), and sporadically bilaterally (2%). Exceptionally there is true agenesis of the hemidiaphragm, but most often the defect is confined to the posterolateral area (Bochdalek hernia). The anterior (Morgagni hernia; 30%) or central areas (2%) are less frequently involved [2]. Occasionally the diaphragm is intact yet thinned and devoid of muscular fibers, and is then called diaphragmatic eventration [3].
Generic 500 mg zithromax fast delivery
Fetoscopic surgery: encouraged by clinical experience and boosted by instrument innovation antibiotics penicillin allergy purchase discount zithromax. Cerebral injury and neurodevelopmental impairment after amnioreduction versus laser surgery in twin-twin transfusion syndrome: a systematic review and meta-analysis infection 5 weeks after abortion purchase cheap zithromax online. Long-term neurodevelopmental outcome in survivors of twin-to-twin transfusion syndrome. Incidence, origin, and character of cerebral injury in twinto-twin transfusion syndrome treated with fetoscopic laser surgery. Long-term developmental follow-up of infants who participated in a randomized clinical trial of amniocentesis vs laser photocoagulation for the treatment of twin-to-twin transfusion syndrome. Short and mediumterm outcomes of live-born twins after fetoscopic laser therapy for twin-twin transfusion syndrome. Outcome following selective fetoscopic laser ablation for twin to twin transfusion syndrome: an 8 year national collaborative experience. Twin-twin transfusion syndrome: neurodevelopment of infants treated with laser surgery. Risk factors for neurodevelopment impairment in twin-twin transfusion syndrome treated with fetoscopic laser surgery. Neurodevelopmental outcome in twin anemia-polycythemia sequence after laser surgery for twin-twin transfusion syndrome. Twin anemia polycythemia sequence: current views on pathogenesis, diagnostic criteria, perinatal management, and outcome. Neonatal morbidity in growthdiscordant monochorionic twins: comparison between the larger and the smaller twin. Cognitive outcome in childhood of birth weight discordant monochorionic twins: the long-term effects of fetal growth restriction. Persistent epigenetic differences associated with prenatal exposure to famine in humans. Umbilical cord occlusion for selective feticide in complicated monochorionic twins:a systematic review of the literature. Selective feticide in complicated monochorionic twin pregnancies using ultrasound-guided bipolar cord coagulation. Radiofrequency ablation for selective reduction in the complicated monochorionic gestation. Pediatric outcome after selective feticide for 30 complicated monochorionic twin pregnancies. Long-term neurodevelopmental outcome after selective feticide in monochorionic pregnancies. Radiofrequency ablation for selective reduction in complex monochorionic multiple pregnancies: A case series. Single fetal demise in monochorionic pregnancies: incidence and patterns of cerebral injury. Fetal brain injury in survivors of twin pregnancies complicated by demise of one twin: a review. Who goes and who stays: subject loss in a multicenter, longitudinal follow-up study. Long-term outcome in twin-twin transfusion syndrome treated with serial aggressive amnioreduction. Neurodevelopmental risks in twin-totwin transfusion syndrome: preliminary findings. Pregnancies complicated by twin-twin transfusion syndrome: outcome and long-term neurological follow-up. Long-term neurodevelopmental outcome in twin-to-twin transfusion syndrome treated with fetoscopic laser surgery. The long term neurologic outcome of children from pregnancies complicated by twin-to- twin transfusion syndrome.
Syndromes
- Something heavy sitting on your chest
- Use of anabolic steroids
- Normal aging changes in the skin
- Lymphoma
- Headache
- Obesity
Purchase zithromax 100mg with amex
This onset of blood flow causes locally high levels of oxidative stress and inhibition of a hypoxic drive to angiogenesis within developing villi; the net effect is regression of the villi over the superficial pole of the sac (*) (corresponding to ** in A) and formation of the chorion laeve antibiotic resistance essay purchase zithromax 100mg with mastercard. The population of proliferating villous cytotrophoblasts slowly increases as gestation advances antibiotic 500mg generic 250 mg zithromax fast delivery, though these cells are dispersed due to growth of the placental villous trees [24]. The outer syncytiotrophoblast is post mitotic and specialized, with an outer brush border that expresses several energy-dependent active carrier systems. At the end of the first trimester, all villi are vascularized and therefore classed as tertiary villi. Pressure of maternal blood is indicated by mmHg in blue and drops across the non-dilated segment of the spiral artery. As the human placenta matures, the volume of syncytiotrophoblast increases due to sustained villous cytotrophoblast proliferation and syncytial fusion. Syncytiotrophoblast nuclei in the near-term placenta tend to aggregate in syncytial knots, in part to facilitate focal thinning of this layer, as vasculosyncytial membrane lacking nuclei, to maximize diffusional exchange. These senescent areas can exhibit some features of apoptosis and a small fraction may shed into maternal blood [36] (reviewed in detail in [37]). Coexistent severe preeclampsia was present in 45% while perinatal mortality occurred in 46%. Most villi however float within the intervillous sapce as branches off the anchoring villi (inset). Since the severely growth-restricted fetus often has low amniotic fluid, the uterine cavity in this context is merely occupied by the small fetus and a much-expanded placenta. However, following delivery, the placenta collapses as maternal blood escapes via ruptured basal plate vessels. Extravillous cytotrophoblasts proliferate in anchoring columns to successfully invade through the decidua (1) and transform the distal spiral arteries (2). These changes mediate high-volume flow at low pressure into the intervillous space (3). The placental villi are covered by the villous trophoblast compartment (4), comprising cytotrophoblasts that proliferate to generate the outer syncytiotrophoblast in direct contact with maternal blood. This type of pathology is termed distal villous hypoplasia, and is commonly associated with severe cytotrophoblast depletion and wave-like syncytial knotting [47]. The net effect of impaired maternal perfusion of these abnormal placental villi is as follows: (1) spiral artery thrombosis may result in wedge infarction of the overlying placental villous trees; and (2) diseased spiral arteries result in uneven placental blood flow, causing ischemia-reperfusion injury to the villi, especially to the delicate outer syncytiotrophoblast in contact with maternal blood [48]. This outer syncytiotrophoblast layer then fails to replenish adequately, due to cell cycle arrest in the cytotrophoblasts [49], resulting in apoptosis [50] or focal necrosis [47]. Second, physiologic placental communication with the mother, which regulates her vascular function via key angiogenic protein signals, becomes impaired, leading to preeclampsia. The de novo production of unique proteins such as serpina-1 [55] can also serve as novel biomarkers. Conversely, the developmentally abnormal placenta, characterized by structurally abnormal villi with defective or damaged areas of syncytiotrophoblast, is prone to thrombosis. We have demonstrated that one or more developmental abnormality of the placenta (small placental size, decidual vasculopathy, abnormal development of placental villi) is seven times more common than any maternal thrombophilia in the context of placental infarction [58]. They are more easily visible than solid areas of placental infarction, but commonly co-exist and are thus indicative of significant placental damage [4]. When basally located, they may dissect spiral arteries and trigger abruption [43]. Increasingly, clinicians now accept that the thrombotic aspects of serious placental disease result from dysregulated hemostasis intrinsic to the placenta, as opposed to a maternal thrombophilia disorder [62]. Typically this is a lethal type of pathology in the early second trimester, however pregnancy continuation and perinatal survival have been reported [73]. The components of these algorithms include clinical characteristics, maternal blood biomarkers, and ultrasound, notably uterine artery (UtA) Doppler. Combining these components as a screening program in a real-time manner is logistically challenging, and therefore mandates both high screening test precision and effective interventions. Note that a consequence of the eccentric cord insertion is failure of the dichotomous branching process to reach across to the opposite quadrant, rendering placental transfer less efficient and reducing birthweight by up to 10%. Note the marginal 2vessel cord and zone of chorionic plate vessel arborization (dashed red circle) that is centered on the cord insertion point.
Purchase genuine zithromax on line
Preliminary experience with endoscopic laser surgery for severe twin-twin transfusion syndrome virus yardville buy cheap zithromax 100mg on-line. Does the source of laser energy influence the coagulation of chorionic plate vessels Emergency cerclage in cases of twin-totwin transfusion syndrome with a short cervix at the time of surgery and relationship to perinatal outcome bacteria journal generic zithromax 500mg free shipping. Laser coagulation of placental anastomoses with a 30 degrees fetoscope in severe mid-trimester twin-twin transfusion syndrome with anterior placenta. Selective laser photocoagulation of communicating vessels in severe twin-twin transfusion syndrome in women with an anterior placenta. Laparoscopically guided uterine entry for fetoscopy in twin-to-twin transfusion syndrome with completely anterior placenta: a novel technique. Fetoscopic laser ablation of placental vessels in severe previable twin-twin transfusion syndrome. A definition of selectivity in laser coagulation of chorionic plate anastomoses in twin-to-twin transfusion syndrome and its relationship to perinatal outcome. Selective versus non-selective laser photocoagulation of placental vessels in twin-to-twin transfusion syndrome. Individual placental territories after selective laser photocoagulation of communicating vessels in twin-twin transfusion syndrome. Appraisal of the selectivity index in a cohort of patients treated with laser surgery for twin-twin transfusion syndrome. Residual anastomoses in twin-to-twin transfusion syndrome treated with selective fetoscopic laser surgery: localization, size, and consequences. The outcome and prognostic factors of twin-twin transfusion syndrome following fetoscopic laser surgery. Sono-endoscopic delineation of the placental vascular equator prior to selective fetoscopic laser ablation in twin-to-twin transfusion syndrome. Severe twin-twin transfusion syndrome: outcome after fetoscopic laser ablation of the placental vascular equator. Fetoscopic laser coagulation for severe twin-to-twin transfusion syndrome: factors influencing perinatal outcome, learning curve of the procedure and lessons for new centres. Endoscopic laser surgery in severe second-trimester twin-twin transfusion syndrome: a three-year experience from a Latin American center. Direct visual control on cord coagulation using a fetoscopy-guided bipolar forceps. Prospective risk of stillbirth and neonatal complications in twin pregnancies: systematic review and meta-analysis. Permanent feto-fetal transfusion from the recipient to the donor twin: a complication of laser surgery in twin-to-twin transfusion syndrome. Endoscopic laser coagulation in the management of severe twin-to-twin transfusion syndrome. Incidence and impact of perioperative complications in 175 fetoscopy-guided laser coagulation of chorionic plate anastomoses in fetofetal transfusion syndrome before 26 weeks of gestation. Incidence of complications in twin-twin transfusion syndrome after selective fetoscopic laser photocoagulation: a single-center experience. Injectible candidate sealants for fetal membrane repair: bonding and toxicity in vitro. Enrichment of collagen plugs with platelets and amniotic fluid cells increases cell proliferation in sealed iatrogenic membrane defects in the foetal rabbit model. In utero acquired limb ischemia in monochorionic twins with and without twin-to-twin trnsfusion syndrome. Twenty-five years of fetoscopic laser coagulation in twinetwin transfusion syndrome: a systematic review. Stage I twintwin transfusion syndrome: rates of progression and regression in relation to outcome.
Purchase 100mg zithromax mastercard
Gene delivery to the hindlimb musculature of the early gestation fetal sheep using ultrasound-guided injection of adenovirus vectors resulted in highly efficient gene transfer prophylactic antibiotics for uti guidelines buy genuine zithromax line, with a low procedure complication rate [18] virus living or not purchase zithromax mastercard. Genodermatoses the genodermatoses are a group of genetic skin diseases that may be associated with significant morbidity and mortality. The genodermatoses may be good candidates for prenatal gene therapy, where gene transfer to the skin via the amniotic fluid may provide obvious advantages over cumbersome postnatal therapy. Transgenic protein expression is seen in the skin after intra-amniotic delivery of adenoviral vectors to mice (12 days post conception [42]), and sheep in the early first trimester (day 33 of 145 days of gestation) using ultrasoundguided injection [18]. In all these studies, only the most superficial layers of the skin, the periderm and epidermis, were transduced. Several strategies have been used in small animals to target the deeper layers, such as intra-amniotic injection with subsequent electroporation [62] or application of microbubbleenhanced ultrasound (shot-gun method) [63, 64]. Injection of lentivirus vectors between days 8 and 12 post conception in fetal mice gives long-term transgenic protein expression in basal epidermal stem cells [65]. Using a skinspecific keratin 5 promoter instead of the cytomegalovirus promoter also improved epidermal gene transfer. Intra-amniotic injection of a recombinant protein that includes the receptor-binding domain of ectodysplasin A in 3 fetuses in the third trimester corrected the phenotype, allowing the neonates to sweat normally [67]. Obstetric Disorders Prenatal gene therapy is being investigated for obstetric disorders. In preterm birth, approximately 40% of cases are preceded by microbial invasion of the intrauterine space, with ascent from the vagina thought to be the most common pathway. Antimicrobial peptides, in combination with mucin and immune cells, constitute a barrier within the cervical canal to prevent ascending infection. Over-expression of human beta-defensin 3, a potent antimicrobial peptide, was targeted to the cervical mucosa of pregnant mice by local vaginal application of the vector in combination with a thermolabile pluronic gel. The transgenic protein expression prevented bacterial ascent from the vagina into the uterine cavity of pregnant mice, suggesting that this approach may be useful in preventing preterm birth in at-risk women [68]. The underlying abnormality in many cases is uteroplacental insufficiency, whereby the normal physiological process of trophoblast invasion that converts the uterine spiral arteries into a high-flow large conduit for blood, fails to occur. Currently there is no therapy available that can improve fetal growth or delay delivery to allow fetal maturity. Abnormally low uterine artery Doppler blood flow and increased vascular resistance is also classically seen in mid gestation. These effects are long term, lasting from mid gestation (80 days) through term (145 days) [71, 72], with reduced intima to media ratios suggesting vessel remodeling and adventitial angiogenesis demonstrated. While this is more invasive than administering oral medication it has the potential advantage of targeting vasoactive drug effects to the maternal uteroplacental circulation. Vectors for Prenatal Gene Transfer An ideal vector for prenatal gene therapy is one that can produce long-term regulated and therapeutic expression of the transferred gene through the use of a single and efficient gene delivery method, and is safe to the mother and fetus, thus allowing incorporation into clinical practice. Less is known about the effect of other viral vectors and non-viral vectors prenatally. Pseudotyping, for example, involves changing the virus capsid (outer covering) for one of a different serotype or of a completely different virus, thus altering its ability to infect particular cell types or organs [78]. The use of different enhancer-promoters can improve gene transfer to specific organs or tissues. These can be derived from the genomes of mammals, viruses, or other organisms, and can even be manipulated to allow regulatable gene expression if required. Removal or modification of virus elements, such as mutating the integrase in lentiviral vectors, renders them incapable of integrating and greatly reduces the risk of insertional mutagenesis. For more detailed information on vectors in relation to fetal gene therapy, the authors refer the reader to other references [79]. It has proven to be difficult, expensive and time consuming to scale up from the small volumes used in laboratory and preclinical studies to the larger amounts needed for clinical trials. Most methods of vector production are based upon adherently growing cells and transient transfection, which is a laborious process. Large-scale viral production has mostly been achieved using a scale-out method, which merely increases the cell-growing surface area in cell factories or cell stacks [80]. This has obvious limitations however, so the development of suspension cell cultures and the use of bioreactors is a further step toward clinical levels of vector production. An additional advantage is the absence of animal origin components in the culture media, as this decreases the likelihood of contamination and is thus advantageous for clinical manufacturing [81].

Buy cheap zithromax 500mg online
Activation of neurohumoral systems: n Release of norepinephrine: It is released by adrenergic cardiac nerves of the autonomic nervous system can antibiotic resistance kill you purchase genuine zithromax line. Norepinephrine increases heart rate infection leg buy zithromax 250 mg without a prescription, myocardial contractility and vascular resistance. This leads to retention of salt and water, with expansion of the interstitial and intravascular fluid volumes (increases circulatory volume) and increases vascular tone. Myocardial structural adaptations: Sustained increase in mechanical work due to pressure or volume overload. Myocardial hypertrophy is a compensatory response to hemodynamic overload and it increases the myocyte contractile strength. This results in concentric hypertrophy (concentric increase in wall thickness) in which the ventricular wall thickness increases without an increase in the size of the chamber. Thus, the best measure of hypertrophy in volume-overloaded hearts is the measurement of the heart weight rather than thickness of ventricular wall. Functional changes: Cardiac hypertrophy is associated with increase in oxygen consumption by heart. The above-mentioned adaptive mechanisms may be adequate to maintain normal cardiac output in the initial phase, but this capacity may be ultimately lost. This causes blood to backup into the lungs ("blood builds up behind the failed heart") producing pulmonary congestion (edema). Increasing pressure in the pulmonary veins is ultimately transmitted back to the capillaries and arteries of the lungs. As hydrostatic pressure increases within the pulmonary veins and capillaries, fluid is forced from the capillaries into interstitial and alveolar spaces. Thus, alveoli contain hemosiderinladen macrophages (so-called heart failure cells). If capillary hydrostatic pressure of pulmonary capillaries exceeds that of plasma osmotic pressure, fluid leaks from capillaries into alveoli and can produce pulmonary edema. Left ventricle is usually hypertrophied and can be dilated (except in failure due to mitral valve stenosis or restrictive cardiomyopathies). Left ventricular dilation can resulting mitral insufficiency and dilatation (enlargement) of left atrium. Microscopy: these changes are nonspecific and consist of hypertrophy of myocyte and variable degree of interstitial fibrosis. Lungs Gross: Due to pulmonary congestion and edema, the lungs become heavy and boggy. Subsequent breakdown of red cells and hemoglobin leads to the liberation of hemosiderin within macrophages. Clinical Features and Complications Symptoms during early left-sided heart failure are as a consequence of pulmonary congestion and edema and may be subtle. Dyspnea (breathlessness or shortness of breath): It occur early and most significant (cardinal) symptom in the progression of left-sided heart failure. Difficulty breathing may be exacerbated by activity (dyspnea on exertion) or lying down (orthopnea and paroxysmal nocturnal dyspnea). As heart failure progresses, worsening pulmonary edema may cause orthopnea [dyspnea when supine (supine position increases venous return from the lower extremities and also elevates the diaphragm), relieved by sitting or standing (hence patients usually sleep in a semi-seated position)] or paroxysmal nocturnal dyspnea (dyspnea usually occurring at night and is a dramatic form of breathlessness, awakening patients from sleep with feelings of suffocation) and dyspnea at rest. Respiratory system: Cough results from bronchial irritation associated with transudation of fluid into air spaces. Cardiovascular system: Cardiomegaly (an enlarged heart), tachycardia, a third heart sound (S3). With progressive dilatation of left ventricles, the outward displacement of papillary muscles causes mitral regurgitation and a systolic murmur. Atrial fibrillation causes stasis of the blood (especially in the atrial appendage) and favors formation of thrombi which can fragment and form emboli. This stimulates the renin-angiotensin-aldosterone axis, increasing intravascular volume and pressures. Unfortunately, these compensatory mechanisms in heart failure, exacerbate the pulmonary edema. It is characterized by symptoms such as irritability, diminished cognition, and restlessness.
Zithromax 500mg for sale
If severe bacteria discovery purchase zithromax amex, chronic passive congestion and edema can develop in the bowel wall and may interfere with nutrient (and/or drug) absorption antibiotic unasyn cheap zithromax 250 mg with amex. Effusion in pleural, pericardial and peritoneal cavities: Systemic venous congestion in rightsided heart failure can lead to transudates (effusions) in the pleural, pericardial or peritoneal cavities (ascites). Subcutaneous tissues: Edema of dependent portions of the body [mainly ankle (pedal) and pretibial edema] is a hallmark of right-sided heart failure. In patients who are chronically bedridden, the edema is mainly found in the presacral region. Clinical Features and Complications Isolated/pure right-sided heart failure usually does not produce respiratory symptoms. These include enlargement of liver and spleen, peripheral edema, pleural effusion, and ascites. Venous congestion and hypoxia of the kidneys and brain due to right-sided heart failure can produce similar changes to that of hypoperfusion of left-sided heart failure. Renal congestion is more severe with right-sided than left-sided heart failure and leads to greater fluid retention and peripheral edema. Typically, it occurs when there is an imbalance between the demand and supply (perfusion) of oxygenated blood. Cardiac myocytes produce energy almost exclusively through mitochondrial oxidative phosphorylation. Hence, cardiac function is dependent on the continuous flow of oxygenated blood through the coronary arteries. Ischemic heart disease: Results due to imbalance between the coronary blood supply and myocardial demand. Variants of Angina Pectoris Stable Angina It is the most common and is also known as typical angina pectoris. Characteristics: Pain is relieved by rest (which decreases demand) or by sublingual nitroglycerin, a strong vasodilator (which increases perfusion). Characteristics: It is of prolonged duration and occurs with minimal physical activity or even at rest. Consequence: May progress to myocardial infarction and is also referred to as preinfarction angina. Unstable (crescendo) Stable angina: Most common type of angina pectoris, substernal chest pain induced by exercise. Write about the etiopathogenesis and pathology of myocardial infarction with diagnostic tests. Age: Its frequency rises progressively with age and peak is between 40 and 65 years of age. It can develop at younger age in patients with major risk factors of atherosclerosis (hyperlipidemia, hypertension, diabetes and cigarette smoking). Sex: Males have significantly higher risk than females mainly during the reproductive period. Other risk factors: Refer under risk factors for atherosclerosis (refer pages 435-7). Decreased/Impaired Coronary Blood Flow Coronary arterial occlusion is the main cause of myocardial ischemia. In these 90% of cases myocardial infarction is due to atherosclerotic narrowing of one or more coronary arteries. The fibrous cap is thin with few smooth muscle cells or groups of inflammatory cells and increased inflammation. Rate of development of occlusion: n Slow progressive occlusion allows time to develop collateral circulation to prevent infarction. Sudden morphological changes in atheromatous plaque It is known as acute plaque change (refer page 460) and is followed by thrombosis, produces unstable angina, myocardial infarction and sudden cardiac death in most of the patients. It may be due to: v Coronary vasospasm without coronary atherosclerosis v Coronary emboli: the source of emboli is thrombi in left side of the heart. These include: n Left atrium in association with atrial fibrillation n Left-sided mural thrombus n Vegetations of infective endocarditis n Intracardiac prosthetic material n Paradoxical emboli: the emboli from the right side of the heart or the peripheral veins, which travel through a patent foramen ovale to the coronary arteries. Increased Myocardial Demand It occurs: v With myocardial hypertrophy v Increased heart rate (tachycardia), increased physical activity, emotional stress, etc. Acute plaque change: It is the sudden change/event occurring in an atheromatous plaque.