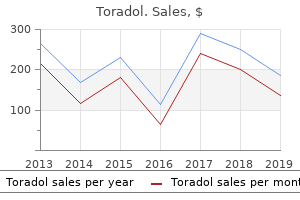
"Buy toradol uk, tailbone pain treatment home remedy".
By: K. Kerth, M.A.S., M.D.
Clinical Director, Touro University Nevada College of Osteopathic Medicine
Buy toradol 10 mg line
Difficulty in climbing stairs arch pain treatment running purchase cheapest toradol, frequent falls blue ridge pain treatment center harrisonburg va discount 10 mg toradol fast delivery, and progressive difficulty in rising from the floor are early features. To rise from the floor, the child may at first need only to push with one hand on a knee. If time is taken to determine the ways in which the weakness interferes with normal activities and uncover the types of tasks that the patient finds difficult, the distribution and severity of muscle weakness can be predicted from the clinical history. Determining the mode of onset and pattern of progression of the symptoms is essential in the differential diagnosis and selection of diagnostic studies. Because many neuromuscular disorders are genetically determined, a complete family history must be obtained. Essential components of the physical examination of patients with neuromuscular disease include inspection, palpation, percussion, evaluation of deep tendon reflexes, and assessment of muscle strength. Inspection can reveal muscle wasting and atrophy (or, conversely, hypertrophy), abnormal spontaneous activity, and abnormal resting postures. Palpation permits assessment of muscle consistency, determination of muscle tone (with observation of resistance to passive motion), and detection of muscle tenderness. Assessment of muscle strength includes individual muscle testing and functional evaluation. A and B, Weakness of the left face with relative sparing of the upper portion secondary to a lesion of the right cerebral hemisphere. There is flattening of the nasolabial fold and inability to retract the corner of the mouth, but the ability to close the eye and wrinkle the forehead is preserved. Weakness of the neck flexors, as evidenced by marked head lag when the child is pulled to sit from the supine position. The abnormally enlarged muscles have an unusually firm, rubbery consistency on palpation. Early in the clinical course, this increase in muscle volume may result from true hypertrophy, with muscle strength proportional to bulk. Later, infiltration by fat and connective tissue sometimes maintains this bulk despite loss of muscle fibers. The onset of symptoms is usually in the second decade, with presenting complaints being foot deformities and gait abnormalities. Often, pes cavus or hammer-toe deformities develop in early childhood long before more overt symptoms appear. The clinical picture is quite variable, and because affected persons often do not consult a physician about their neurologic complaints, the majority of cases remain undiagnosed. The astute physician considers the diagnosis when a patient who presents with unrelated symptoms is found to have pes cavus or hammer-toes and symmetrical distal weakness. The intrinsic muscles of the foot are often affected first, followed by involvement of the peroneal, anterior tibial, long toe extensor, intrinsic hand, and gastrocnemius muscles. Weakness and atrophy may even spread to the more proximal muscles of the leg and forearm. However, as weakness of the extensors of the hips becomes more pronounced, rising from the floor becomes increasingly difficult and requires the use of the hands to "climb up the legs" (the Gower maneuver). Progressive gluteal weakness leads to the assumption of a compensatory posture characterized by a broadened base, accentuated lumbar lordosis, and forward thrusting of the abdomen. There is marked laxity of the shoulder girdle musculature associated with upward displacement of the shoulders and abnormal rotation of the scapulae. This series of diagrams illustrates the sequence of postures used in attaining the upright position by a child with Duchenne muscular dystrophy. A to C, First, the legs are pulled up under the body, and the weight is shifted to rest on the hands and feet. D, the hips are then thrust in the air as the knees are straightened, and the hands are brought closer to the legs. A, this child, age 5, demonstrates weakness and hypotonia of the shoulder girdle musculature.
Buy toradol uk
The success rate of air enema reduction has been reported to be as high as 94% but is very operator dependent and must be performed by an experienced radiologist chronic pain medical treatment guidelines 2012 cheap toradol. Those patients who have an incomplete or failed reduction pain management for old dogs generic toradol 10mg amex, and who are clinically well, may undergo a repeated attempt at air reduction in the appropriate setting. The ileum is pulled through the ileocecal valve into the colon, the most common pattern seen in infancy, pictured here. Upper gastrointestinal studies should be avoided in these patients secondary to aspiration risks. It is important to remember that these patients can present along a spectrum of severity of illness. Like many patients with bowel obstructions, they may be extremely dehydrated and therefore must be volume resuscitated prior to attempts at reduction. Some have also argued that it is important to give antibiotics prior to attempts at reduction, because the reduction can precipitate bacterial translocation and bacteremia. If the patient presents late in the course of the disease, they may have clear evidence of peritonitis, and an attempt at enema reduction should not take place. The risk of recurrent intussusception after radiologic guided air enema is reported to be around 5% to 7% with one-third recurring within the first 24 hours and most recurring within the first few days. Patients with recurrent symptoms should have a repeat ultrasound and an attempt at enema reduction if positive. Ileoileal and jejunoileal intussusceptions are generally too proximal to be amenable to radiographic reduction. If the intussusceptions have a short segment, they may be physiologic; or if they have a longer segment or are symptomatic, they may be due to a mechanical lead point that would require surgery. Postoperative intussusception may also occur in the small bowel and requires operative reduction. Twisting and compression from postoperative adhesions, amniotic bands, omphalomesenteric (vitelline) remnants. The most common cause of intestinal obstruction is adhesions from previous surgery, intraabdominal infection, and trauma. Early nasogastric decompression and aggressive rehydration may alleviate the symptoms, halt the progression of distension, and give time for resolution of the obstruction. Failure of resolution, progression of symptoms, or lack of any prior risk factor for obstruction should prompt surgical exploration. Gastrointestinal Bleeding Gastrointestinal bleeding accounts for roughly three out of every 1000 pediatric emergency room visits. The evaluation involves a careful assessment of several important factors and the establishment of a management protocol (Table 18. Free reflux of contrast into the bowel proximally signals complete reduction of the intussusception. Those patients in acute or impending hypovolemic shock require urgent stabilization. In cases of more chronic or subacute blood loss, symptoms of anemia, fatigue, and pallor are more common. A thorough history and physical examination in conjunction with serologic, radiologic, and endoscopic studies are critical to ascertain the etiology of the bleeding. The duration, severity (amount), previous episodes, and location of the source of the bleeding are among the most important historical factors. Drug ingestion, exposure to sick contacts, inherited coagulopathies, vitamin deficiency, congenital or acquired liver dysfunction, or family history of chronic intestinal disorders may shed further light on the source of bleeding. Severe acute blood loss may be associated with both upper (hematemesis) and lower (hematochezia or melena) bleeding. Infants Swallowed maternal blood during childbirth or from cracked nipples during breast-feeding is commonly mistaken for gastrointestinal bleeding in the newborn. The Apt-Downey test differentiates between maternal and fetal blood in the newborn and should be performed to identify the source of the blood. This is a rare occurrence because of strict delivery room protocols; however, infants who are unstable or urgently transferred from the delivery room to other institutions, or whose parents refuse vitamin K injection, may be at greatest risk. The delivery room records for all newborns who present with upper gastrointestinal bleeding should be examined for vitamin K administration.
Buy 10mg toradol fast delivery
Large lacerations phantom pain treatment 10 mg toradol amex, through-and-through lacerations topical pain treatment for shingles cheap 10 mg toradol amex, and those associated with extensive, recurrent, or uncontrolled bleeding require careful assessment and surgical closure. To reduce risk of infection, saline irrigation and antimicrobial prophylaxis are indicated for all intraoral lacerations, regardless of whether sutures are required. Traumatic Ulcers Painful ulcerations may result from mechanical, chemical, or thermal trauma. Injury may be secondary to irritation by objects, trauma during mastication, toothbrush trauma, or abnormal habits. Large ulcerations involving the buccal mucosa or lower lip may be associated with cheek or lip biting after inferior alveolar nerve block. Lesions usually heal without scarring, but secondarily infected lesions may require antibiotic therapy. Identification and elimination of the habit is necessary for resolution of habit-related lesions. In this radiograph the condyles bend inward at nearly 90 degrees above the fracture lines. Patients undergoing chemotherapy are encouraged to brush two or three times per day with a soft bristle toothbrush. If a patient develops oral mucositis, chlorhexidine may need to be discontinued because its high alcohol content may dehydrate the tissue. It is also important for patients undergoing chemotherapy to supplement fluoride because of the possibility of xerostomia (dry mouth), which may lead to increased caries risk. Trauma to the Dentition As noted earlier, facial injuries in childhood frequently involve the dentition and supporting bones. One prospective study showed that 50% of children had suffered at least one dental injury by age 14. Although falls are the major source in early childhood, bicycle and skateboard accidents, contact sports, fights, and motor vehicle accidents become more prevalent with advancing age. The risk of facial injuries is relatively high in (1) children with neurologic disorders that impair coordination; (2) children with protruding maxillary anterior teeth; (3) children with a deviant anatomic relationship, such as an anterior open bite or a hypoplastic upper lip; and (4) 2- to 3-year-old children with immature motor skills and coordination. Falling while a child is actively using a bottle, sippy cup, or pacifier is associated with more traumatic dental injuries. A, A large gaping tongue laceration in a toddler produced by the upper front teeth being forced through the tissue by a fall with the tongue protruded. B, this small laceration, although gaping slightly, does not require surgical closure. In this site, delayed hemorrhage after separation of the eschar and deformity with scarring are particular problems. Potential Complications Pulp hemorrhage and/or vasodilation of the pulp vessels are a common response to concussive injury to a tooth and can lead to development of discoloration within 10 to 14 days. Excessive pulpal vasodilation can actually result in pressure necrosis of the pulp. Injuries that produce loosening or displacement of a tooth disrupt the anchoring periodontal ligament. If disruption is mild, there may be no sequelae, although in some cases it stimulates overactive bony repair, ankylosing the tooth in place. When disruption is more severe, the neurovascular bundle can be torn, resulting in pulpal necrosis, which then may lead to abscess formation. Finally, dental fractures in which dentin and/or pulp are exposed open a pathway for bacteria and may lead to abscess formation. Several extensive classifications of tooth injuries have been suggested, but for the purpose of this text a more simplified descriptive classification is presented. However, any fracture of the crown that results in exposure of the dentin requires emergency treatment to prevent infection and subsequent pulp necrosis. The treatment of choice is to seal the exposed dentin with calcium hydroxide and protect it with an acid-etched resin bandage. As noted earlier, dental fragments are occasionally embedded in the soft tissues of the lip or tongue; therefore appropriate examination and palpation of these areas are indicated. Crown Fractures With Pulpal Exposure Fractures that traverse all three tooth layers to expose the pulp usually involve a significant loss of tooth structure. On physical examination, the fracture surface reveals the pink central pulp surrounded by the beige dentinal layer. Severe vertical or diagonal fractures may also result in pulp exposure and can at times extend to involve the root.
Toradol 10mg otc
An exodeviation may be controlled by fusion (exophoria) pain medication for dogs with bite wounds purchase 10mg toradol otc, be manifest intermittently (intermittent exotropia) back pain treatment kerala buy discount toradol 10mg line, or be constant (exotropia). Intermittent exodeviations may become manifest with fatigue, daydreaming, or illness. Patients with exodeviations frequently squint one eye in bright light, but they typically do not experience the pupillary light is centered. It appears as if the right eye is esotropic but the light reflex remains centered in the pupil. This may cause symptoms of discomfort while reading, complaints of images jumping or moving, or intermittent diplopia at near range. To test for convergence insufficiency, the child is asked to fixate on a target with detail as it is brought progressively closer. If the eyes converge, and then break their alignment and diverge at a distance greater than 10 cm from the eyes, the patient should be evaluated for convergence insufficiency. With cover and uncover testing, an exodeviation will be seen at near fixation, and it will be smaller or not seen at distance fixation. Because young children do not complain of monocular vision loss, especially if congenital or with onset during infancy, sensory strabismus is frequently the presenting sign of vision loss caused by pathology of the retina or optic nerve. When the macula is displaced temporally, the eye rotates outward to align its visual axis on the fixation target. This appearance is caused by a temporal displacement of the fovea, usually due to cicatricial changes of the retina after retinopathy of prematurity. Third (Oculomotor) Cranial Nerve Palsy the third cranial nerve innervates the medial rectus muscle. In third nerve paralysis, the action of the lateral rectus muscle, innervated by the sixth cranial nerve, is unopposed and produces an exodeviation. The third nerve also innervates the superior and inferior recti; the inferior oblique muscles; the levator palpebrae superioris, which elevates the lid; the ciliary muscle, which is responsible for accommodation of the lens; and the iris sphincter muscle, which produces miosis of the pupil. In the presence of a complete third cranial nerve palsy, the eye assumes a down and outward position, the eyelid is ptotic, and the pupil is enlarged. The most common causes for acquired third nerve paralysis in children are trauma and tumor. Normal vascular pattern Fovea Vertical deviations may occur in only one field of gaze, or they may be comitant, the same, in all fields of gaze. Vertical deviations may have a cyclotorsional component and be associated with a head tilt or head posture to eliminate double vision. All patients with torticollis should be evaluated for cyclovertical muscle palsies. The most common cyclovertical deviation is due to a palsy of the fourth cranial (trochlear) nerve. The forced opening of tightly closed eyelids will reveal an upward, slightly outward movement of the eye under the closed eyelids (normal Bell response). Other features are elevation of the eye and difficulty depressing the eye in adduction. Children with congenital fourth nerve palsies usually do not have complaints of diplopia; but if they are asked about diplopia when their eyes are in the contralateral field of gaze, especially up and away from the paretic side, they can recognize the presence of diplopia. Later in life, patients with congenital fourth nerve palsy may decompensate in their control of the deviation and develop symptomatic diplopia. Some subtle facial asymmetry, especially of the cheek and jaw line, is almost always seen in congenital cases as the children age. Review of candid photos will frequently display consistently repeated head tilts that usually have not been noticed by the family. Brown syndrome describes an isolated motility disorder in which there is an inability to elevate the eye when in adduction. This may be caused by a congenital anomaly of the superior oblique tendon, or it may be acquired as an idiopathic inflammation or tenosynovitis of the superior oblique tendon. Double elevator palsy is an inherited unilateral or bilateral condition in which there is hypotropia and limitation of elevation of the involved eye. To achieve binocularity, patients tilt their chins up and position their heads back. In primary (straight ahead) gaze (A) and right gaze (B), the eyes are well aligned.
Toradol 10mg with amex
When bilateral pain treatment center utah purchase toradol canada, these renal disorders may present early in life with poor weight gain pain treatment center of greater washington justin wasserman order toradol 10 mg on-line, pallor, emesis, and tachypnea resulting from metabolic acidosis. Urine output is often maintained or increased due to concentrating defects, but correlates poorly with renal function reflected by the serum creatinine level. Renal hypoplasia is often an isolated disorder without other systemic or genitourinary tract anomalies, whereas obstruction of the gastrointestinal or genitourinary tract occurs frequently in children with renal dysplasia. Less common anomalies may include trisomy 21, tracheoesophageal fistula, ventricular septal defect, and lumbosacral dystrophies. Cystic dysplasia may be a major component of several syndromes with distinct additional malformations (see Table 14. The overall risk for siblings of children with isolated forms of dysplasia or hypoplasia is usually less than 10% but is generally higher than the general population if one of the parents has renal aplasia or other structural kidney disease. MulticysticDysplasia Multicystic dysplasia, usually unilateral, is the most common cystic disorder in children, as well as the most common cause of abdominal mass in newborns. Multicystic dysplasia represents an extreme case of renal cystic dysplasia in which there is complete loss of the normal renal architecture with microscopic primitive ducts, fibrosis, islands of ectopic cartilage, and usually ureteral atresia. This condition is most commonly discovered by prenatal ultrasonography, or it may be diagnosed during the neonatal period after palpation of a "lumpy" intraabdominal mass of variable size that often transilluminates. The parenchyma in the upper pole is normal, but microscopic examination of the lower pole showed several morphologic features of dysplasia. Very large multicystic kidneys can interfere with respiration or produce mechanical intestinal compression. Radionuclide scanning and renal ultrasonography are usually sufficient to establish the diagnosis. The unaffected contralateral kidney is usually hypertrophied and has normal corticomedullary differentiation and no evidence of obstruction. Obstructive disorders, such as posterior urethral valves, urethral atresia, or ureteroceles obstructing a duplicated ureter draining the upper pole, may be associated with morphologic features of dysplasia. However, correction of any associated obstructive abnormalities that may be present in the contralateral kidney is of vital importance. AlportSyndrome Alport syndrome, or hereditary nephritis, is transmitted most commonly via X-linked inheritance and more rarely autosomal recessive or autosomal dominant inheritance with variable penetrance. Frequently less severe mutations, such as point mutations, result in less severe disease than truncating mutations that typically lead to more severe disease. The classic clinical presentation of Alport syndrome is persistent or recurrent gross hematuria that may be evident in early childhood. Proteinuria is absent or mild in the early stages of the disease but is invariably present as the disease progresses. The majority of individuals with Alport syndrome have neither deafness nor ocular defects. Alport syndrome must be differentiated from several benign causes of childhood hematuria, including thin glomerular basement membrane disease, and other progressive glomerular disorders. Diagnosis relies on careful family history, genetic testing, audiologic or ocular abnormalities, renal histopathologic features (such as, the presence of foam cells) and glomerular sclerosis on light microscopy. Polyuria and polydipsia resulting from a urinary concentration defect and, at times, severe salt wasting are prominent clinical features. HypophosphatemicRickets Rickets is a disturbance of growing bone in which defective mineralization of the matrix leads to an abnormal accumulation of uncalcified cartilage and osteoid. The characteristic radiologic features of hypophosphatemic rickets, as in all forms of childhood rickets, include early widening of the spaces between the end of the metaphyses of long bones and an overall decrease in bone density. Biochemical differentiation from other forms of rickets consists of hypophosphatemia, normal plasma calcium and bicarbonate levels, normal parathyroid hormone and 1,25-dihydroxyvitamin D levels, and absence of aminoaciduria. Management aims to promote healing of the rickets and to increase growth velocity through improvement of serum phosphorus and alkaline phosphatase concentrations through the judicious combined use of oral phosphate and calcitriol while avoiding hypercalcemia, hypercalciuria, hyperoxaluria, and hyperparathyroidism. Sequential biochemical and renal ultrasonographic monitoring is essential in determining the lowest amounts of oral phosphate and calcitriol doses that achieve the treatment objectives while minimizing complications, such as nephrocalcinosis. It is characterized by body-wide intralysosomal accumulation of cysteine, which consists of di-sulfide bonded cysteine monomers.
Radix Aucklandiae (Costus). Toradol.
- Dosing considerations for Costus.
- Are there safety concerns?
- How does Costus work?
- What is Costus?
- Worm (nematode) infections, digestive problems, gas, asthma, cough, dysentery, and cholera.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96828
Buy toradol visa
Removal is assisted by use of a weak vinegar rinse (which is left on under a shower cap or towel for 15 to 20 minutes) midwest pain treatment center fremont ohio purchase toradol 10 mg free shipping, followed by combing with a fine-toothed comb pain swallowing treatment purchase 10mg toradol mastercard. This is important because the persistence of dead nits is a common cause of misunderstanding by school health care workers, who insist on re-treating the children or sending them home from school. Active disease is present only if a viable organism or new nits attached close to the scalp are identified. Diagnosis of pediculosis must be considered in patients with unexplained scalp pruritus. Lice are six-legged insects visible to the unaided eye; they are commonly found on the scalp, eyelashes, and pubic areas. They are best identified close to the skin or scalp, where they can be seen moving around and where their eggs are more numerous and more obvious. Diagnosis can be made either by identifying a louse or by plucking hairs and confirming the presence of nits by microscopic examination. Eradication of lice requires application of a pediculicide to infested hair-bearing areas of all household members and cleaning measures similar to those specified for ridding the house of scabies. Resistance to many over the counter pediculicides has been documented worldwide, and some cases may require multiple treatments or use of new prescription agents. A permethrin 1% to 5% cream rinse is an appropriate first-line treatment, but if cure is not achieved and resistance is suspected, malathion lotion or topical ivermectin lotion are both highly effective second-line options. However, it is important to instruct patients to avoid smoking near the patient, because malathion is flammable. Four percent benzoyl alcohol lotion has been approved, and a number of new products are in the pipeline. Lindane, an agent used in the past, is contraindicated for use in infants, children, and the elderly because of the potential for systemic absorption and neurotoxicity. Lesions may appear on the face as early as infancy, although they usually begin to develop in the second decade of life during the onset of puberty. Other areas with prominent sebaceous follicles including the upper chest and back may be involved as well. However, abnormalities in follicular keratinization are thought to produce the earliest acne lesion, the microcomedone. In time, microcomedones may grow into clinically apparent open comedones (blackheads). The entire process is driven by androgens, which stimulate sebaceous gland differentiation and growth and the production of sebum. The proliferation of Propionibacterium acnes in noninflammatory comedones and the rupture of comedone contents into the surrounding dermis may trigger the development of inflammatory papules, pustules, and cysts. Cystic acne is typified by nodules and cysts scattered over the face, chest, and back. Acne fulminans is a rare subtype of inflammatory acne that can appear rapidly and in conjunction with fever and joint pain. This should be referred immediately to a pediatric dermatologist, because it requires careful use of systemic therapy and close systemic monitoring. Although therapy must be individualized, patients with mild to moderate comedonal and/or inflammatory acne usually respond well to a combination of topical retinoids, benzoyl peroxide, and antibiotics. Moderate to severe papulopustular acne warrants the use of oral antibiotics in combination with topical agents. The authors recommend prompt referral to a pediatric dermatologist in cases of moderate or severe acne that are not responding to first-line therapy in 2 to 3 months, because scarring can happen quickly in these patients and more aggressive definitive therapy should be considered early in its course. Fortunately, primary skin cancer is relatively rare in childhood, and most tumors and infiltrative lesions are benign. B, Comedonal acne with closed comedones, or whiteheads, on the forehead, accentuated by side lighting. C, Papulopustular acne with inflamed papules and pustules over the cheeks, which responded well to antibiotics. D, Cystic acne shows deep cysts with marked erythema that can cause severe scarring.
Buy 10mg toradol with amex
There may be associated nausea and vomiting pain medication for dogs rimadyl order cheap toradol, but most children do not appear acutely ill pain medication for little dogs buy cheapest toradol. Progressive papilledema may lead to optic atrophy, and treatment is essential to prevent loss of vision. Neurocysticercosis Neurocysticercosis is another disorder that can present with signs of increased intracranial pressure. Neurocysticercosis is being seen with increasing frequency in developed countries, often in immigrants from or recent visitors to endemic areas. The portion of the facial nerve nucleus that supplies the lower half of the face receives predominantly crossed fibers originating from the opposite cerebral hemisphere; the portion that innervates the upper half receives fibers from both cerebral hemispheres. Flaccid weakness of the entire left face resulting from a lesion of the left facial nerve. A, Flattening of the nasolabial fold and inability to retract the corner of the mouth. Causes of peripheral facial weakness include infection, trauma, hypertension, a cerebellopontine angle mass, tumors of the pons, and acute idiopathic paralysis (Bell palsy). Functional evaluation of muscle strength is accomplished by observing the patient rising from the floor, rising from a chair, stepping onto a stool, climbing stairs, walking on the heels, hopping on the toes, and raising the arms above the head. This evaluation permits rapid detection of proximal weakness of the hips and shoulders and distal weakness of the legs. Central Facial Weakness With a lesion above the level of the facial nerve nucleus. The ability to wrinkle the forehead (frontalis muscle) and to voluntarily close the eyes (orbicularis oculi muscle) is preserved. Duchenne Muscular Dystrophy the muscular dystrophies are genetically determined disorders characterized by progressive degeneration of skeletal muscle, usually after a latency period of seemingly normal development and function. The various clinical types of muscular dystrophy are traditionally classified on the basis of patterns of inheritance, distribution of initial weakness, age of onset of clinical manifestations, and rate of progression (Table 16. Duchenne muscular dystrophy, affecting 1 in 3500 male births, is characterized by X-linked recessive inheritance; early onset; symmetrical and initially selective involvement of pelvic and pectoral girdles; pseudohypertrophy of the calves; high levels of activity of certain serum enzymes, notably creatine kinase; and relentless progression leading to wheelchair confinement by adolescence and death from cardiorespiratory insufficiency by 20 years old. Duchenne muscular dystrophy is caused by a deletion mutation affecting the Xp21 region on the short arm of the X chromosome. Dystrophin, the large cytoskeletal protein normally encoded by this gene locus, is absent from the muscle fibers of patients with Duchenne muscular dystrophy. The precise function of dystrophin in maintaining the integrity of muscle and the mechanism by which dystrophin deficiency produces progressive muscle destruction remain to be determined. Becker muscular dystrophy, an allelic disorder affecting 1 in 30,000 male births, is distinguished clinically by later age at onset, slower rate of progression, and longer survival and biochemically by the presence of dystrophin of abnormal molecular weight. Clinical manifestations of Duchenne muscular dystrophy do not usually appear until the second year of life or later. Early developmental milestones are normally attained, although the first attempts at walking may be delayed. Gait is often clumsy and awkward from the start, and the ability to run is never normally attained. These brothers, ages 5 and 8, show the progression of compensatory postural adjustments with broadening of stance, accentuated lumbar lordosis, and forward thrusting of the abdomen, all more pronounced in the older boy. With involvement of the distal upper extremities, there may be obvious wasting of the intrinsic hand muscles and development of secondary "claw-hand" deformities. Deep tendon reflexes are lost first in the gastrocnemius and soleus muscles, and subsequently in the quadriceps femoris muscle and upper limbs. Congenital Cervical Spinal Atrophy Congenital cervical spinal atrophy is a rare disorder that is manifested at birth by dramatic flaccid paresis of the upper extremities. The presence of congenital flexion contractures suggests chronic denervation that must have occurred in utero and allows this syndrome to be distinguished from injury to the cervical spine or brachial plexuses during delivery (see Chapter 2). Abnormalities in the formation of the transverse palmar creases are present in all cases. However, as activity continues, the child begins to walk freely and with adequate "warm-up" can run without difficulty. Generalized muscular hypertrophy is a frequent finding on examination, with affected children often having an unusually welldeveloped, athletic appearance. This belies their sedentary habits and physical ineptitude resulting from muscle stiffness. Clinically, myotonia may be demonstrated by observing delayed relaxation of the muscles after sustained voluntary contraction, such as clenching of the hand.
Purchase toradol 10 mg online
B pain medication for dogs arthritis order toradol 10 mg without prescription, In this case pain treatment center connecticut purchase toradol 10mg visa, the bowing was caused by a congenital pseudarthrosis of the tibia, a condition frequently associated with neurofibromatosis 1 (see Chapter 16). Unilateral bowing is not a result of intrauterine positioning and should prompt investigation for an underlying disorder. Genu Valgum (Physiologic Knock-Knee) Genu valgum, or knock-knee, is a normal variation of lower extremity configuration, generally noted in children between 3 and 5 years old. The phenomenon is part of the normal process of remodeling of the lower extremities during growth and development. It is more frequently seen in females and may be associated with ligamentous laxity. While standing, the child is noted to have an increased distance between the feet when the medial aspects of the knees touch one another. Not uncommonly, the child will place one knee behind the other in an attempt to get the feet together. In some cases, valgus alignment of the feet and a pes planus deformity may be noted. Radiographs reveal no osseous or physeal abnormalities, but accentuation of the angular deformity of the knee secondary to ligamentous laxity is seen on weight-bearing views. One must rule out the possibility of an underlying metabolic condition, such as rickets or renal disease. Treatment is generally not indicated, because the condition gradually corrects with time. On careful examination, a localized angular deformity of the proximal tibia is apparent. In general, there is no evidence of the ligamentous laxity commonly associated with physiologic bowing. Radiographs reveal fragmentation of the medial epiphysis of the tibia associated with beaking and loss of height in this region, as well as the characteristic angular deformity. A satisfactory response Blount Disease Blount disease is an isolated growth disturbance of the medial tibial epiphysis manifested as an angular varus deformity of the proximal tibia with apparent progressive genu varum. The etiology of this condition is unknown, although it appears to be more common in African Americans. It may represent a compression injury to the medial growth plate of the proximal tibia. A, this patient has a unilateral angular deformity of the proximal left tibia that gives the appearance of genu varum. B, Both proximal tibias are bowed in another patient as a result of fragmentation and loss of height of the medial epiphyses. C, this radiograph shows the typical fragmentation, loss of height, and angular deformity or beaking of the medial portion of the proximal tibia. Popliteal (Baker) Cyst Popliteal cysts occurring in childhood are encountered most commonly in children between 5 and 10 years old and occur significantly more frequently in boys than in girls. They are located in the posteromedial aspect of the knee joint in the region of the semimembranosus tendon and medial gastrocnemius muscle belly. Pathologically, a fibrous tissue or synovial cyst filled with synovialike fluid is seen. In contrast to those seen in adults, popliteal cysts in childhood generally do not communicate with the joint capsule but originate instead beneath the semimembranosus tendon, presumably as a result of chronic irritation. On occasion vague pain is noted, but evaluation is usually sought because of a recently noted painless mass. On examination, a soft, nontender, cystic mass is found in the described location. Range of motion of the joint is normal unless the cyst is particularly large, limiting flexion. Popliteal cysts are benign and may resolve over time, although surgical excision is reasonable if desired. Osgood-Schlatter Disease Osgood-Schlatter disease is a traction apophysitis of the tibial tubercle that tends to develop during the adolescent growth spurt. It is thought that differential rates of growth in the osseous and soft tissue structures and stress on the apophyses produced by vigorous physical activity are contributing factors.
References: