"Generic geriforte 100mg with amex, herbals vs pharmaceuticals".
By: J. Mufassa, MD
Associate Professor, Duke University School of Medicine
The association between pubertal status and sleep duration and quality among a nationally representative sample of U himalaya herbals 52 purchase geriforte without prescription. Diurnal rhythms of luteinizing hormone herbs philipson cheap geriforte 100mg, follicle-stimulating hormone, and testosterone secretion before the onset of male puberty. Diurnal rhythms of luteinizing hormone, follicle-stimulating hormone, testosterone, and estradiol secretion before the onset of female puberty in short children. Developmentally delimited emergence of more orderly luteinizing hormone and testosterone secretion during late prepuberty in boys. Hypothalamic-pituitary regulation of puberty in man: evidence and concepts derived from clinical research. Serum luteinizing hormone rises within minutes after depot leuprolide injection: implications for monitoring therapy. A single luteinizing hormone determination 2 hours after depot leuprolide is useful for therapy monitoring of gonadotropin-dependent precocious puberty in girls. Comparison of detection of normal puberty in boys by a hormonal sleep test and a gonadotropin-releasing hormone agonist test. Use of local data to enhance uptake of published recommendations: an example from the diagnos- 231. Time course of the serum gonadotropin surge, inhibins, and anti-mullerian hormone in normal newborn males during the first month of life. Plasma testosterone-binding affinity and testosterone in umbilical cord plasma, late pregnancy, prepubertal children and adults. Serum anti-mullerian hormone concentrations are elevated in oligomenorrheic girls without evidence of hyperandrogenism. The pubertal growth spurt in eight patients with true precocious puberty and growth hormone deficiency: evidence for a direct role of sex steroids. A syndrome of female pseudohermaphrodism, hypergonadotropic hypogonadism and multicystic ovaries associated with missence mutations in the gene encoding aromatase (P450 arom). Estrogen replacement therapy in a man with congenital aromatase deficiency: effects of different doses of transdermal estradiol on bone mineral density and hormonal parameters. Determinants of growth during gonadotropin-releasing hormone analog therapy for precocious puberty. Importance of estrogen on bone health in Turner syndrome: a cross-sectional and longitudinal study using dual-energy X-ray absorptiometry. The contribution of testosterone to skeletal development and maintenance: lessons from the androgen insensitivity syndrome. Gender and sexual maturationdependent contrasts in the neuroregulation of growth hormone secretion in prepubertal and late adolescent males and females: a general clinical research center-based study. Augmentation of growth hormone secretion after testosterone treatment in boys with constitutional delay of growth and adolescence: evidence against an increase in hypothalamic secretion of growth hormone-releasing hormone. Somatomedin-C in normal puberty and in true precocious puberty before and after treatment with a potent luteinizing hormone-releasing hormone agonist. Serum levels of growth hormone binding protein in children with normal and precocious puberty: relation to age, gender, body composition and gonadal steroids. Syndrome of precocious menstruation and galactorrhea in juvenile hypothyroidism: an example of hormonal overlap in pituitary feedback. Hypothalamic control of the pituitary-gonadal axis in higher primates: key advances over the last two decades. Recent discoveries on the control of gonadotrophin-releasing hormone neurones in nonhuman primates. Inhibition of luteinizing hormone secretion by testosterone in men requires aromatization for its pituitary but not its hypothalamic effects: evidence from the tandem study of normal and gonadotropin-releasing hormonedeficient men. Firing pattern and rapid modulation of activity by estrogen in primate luteinizing hormone releasing hormone-1 neurons. Colocalization of kisspeptin and gonadotropin-releasing hormone in the ovine brain. Age-dependent elevations in plasma kisspeptin are observed in boys and girls when compared with adults. Postnatal remodeling of gonadotropin-releasing hormone I neurons: toward understanding the mechanism of the onset of puberty.
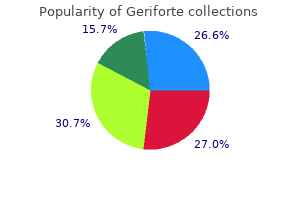
Cafe de Bugre (Cha De Bugre). Geriforte.
- How does Cha De Bugre work?
- Are there safety concerns?
- Weight loss and obesity, reducing cellulite, cough, edema, gout, cancer, herpes, viral infections, fever, heart disease, and wound healing.
- Dosing considerations for Cha De Bugre.
- What is Cha De Bugre?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97068
Growth can be retarded in children with asthma herbals and liver damage buy cheap geriforte 100 mg, including those who have not received glucocorticoid therapy herbs used in cooking discount geriforte 100 mg online. However, despite this growth impairment, there is at most only a small difference in final height achieved by those with asthma, with the majority of the growth failure due to a delay in puberty. Intermittent glucocorticoid therapy is usually not associated with impaired final height. Alternate-day or aerosolized glucocorticoid therapy often ameliorates growth retardation and can be associated with an accelerated catch-up phase. The linear growth rate during childhood is generally normal before puberty,709 followed by delayed puberty, including a delayed and attenuated pubertal growth spurt. Alterations of vitamin D metabolism, while potentially affecting skeletal mineralization, do not diminish growth. In addition, some measures of lung function are slightly improved, notably forced vital capacity, although this improvement did not always exceed that expected based on the improved growth. Specifically, there has not been an increase in glucose intolerance or diabetes mellitus, although in some studies fasting glucose levels were increased. Poor growth is a characteristic feature of chronic inflammatory disease and recurrent serious infection. With proper treatment, however, children with congenital hypothyroidism reach a height appropriate for their genetic potential. Growth failure may be the most prominent manifestation of hypothyroidism in children. Skeletal maturation is delayed in those children in whom the hypothyroidism was sufficient to retard growth, with the bone age at diagnosis corresponding to the age at onset of the hypothyroidism. Although chronic hypothyroidism is usually associated with delayed puberty, precocious puberty and premature menarche can occur in hypothyroid children (see Chapter 13). In those children with severe growth failure, treatment with thyroid hormone results in rapid catch-up growth. In cases of prolonged severe hypothyroidism, the advancement of skeletal maturation with treatment can exceed the growth acceleration, resulting in a compromised adult height. Untreated severe congenital hypothyroid- with the duration of hypothyroidism before initiation of treatment. Catch-up growth may be particularly compromised if therapy is initiated near puberty. Children with hyperthyroidism present with an increased height and advanced bone age. However, despite the advanced bone age at diagnosis, the final height of children treated for hyperthyroidism remains normal in relation to genetic potential. This type of growth retardation has become increasingly rare with modern diabetes care. Chronic metabolic control did not correlate with the pubertal height gain or with the normal final height. Nevertheless, good glycemic control may improve growth at certain maturational periods such as puberty. Glucocorticoid excess impairs skeletal growth, interferes with normal bone metabolism by inhibiting osteoblastic activity, and enhances bone resorption. Even modest doses of oral glucocorticoids can inhibit growth; these doses may be as low as 3 to 5 mg/m2 per day of prednisone or 12 to 15 mg/m2 per day of hydrocortisone. Alternateday glucocorticoid treatment decreases but does not eliminate the risk of growth suppression. However, inhaled corticosteroids do not appear to significantly impair final height. In addition, Cushing syndrome in children may not cause all the clinical signs and symptoms associated with the disorder in adults and may manifest with growth arrest. This condition is discussed in detail in Chapter 28 but is included here because short adult height is a common feature. He had onset of rapid weight gain associated with a decrease in linear growth velocity at age 7. The diagnosis was made, and an adrenalectomy (arrow) was performed at age 9 12 years, with an almost immediate increase in growth rate and striking catch-up growth.

Autophosphorylation appears to occur by transphosphorylation of sites on the opposite -subunit equine herbals nz discount geriforte online visa. This process then activates downstream phospholipid signal transduction pathways that include Akt herbs n more cheap geriforte 100mg on line. Activation of Akt leads to regulation of diverse cellular processes including apoptosis, glucose transport and metabolism, protein synthesis, mitosis, and differentiation. Studies thus far have been performed in vitro, and thus, the in vitro significance of the binding characteristics is not known. The receptor does not contain an intrinsic tyrosine kinase domain or any other recognized signal transduction mechanism. Exons 1 through 46 encode the extracellular region of the receptor, which contains 15 repeat sequences of 147 residues each. Exons 47 and 48 encode the 23-residue transmembrane domain and a small cytoplasmic domain consisting of only 164 residues. Postnatally, mice with deletion of Igf1 who survive the neonatal period continue to have growth failure, with weights 30% of normal by 2 months of age. Igf1-/-, Igf1 gene null mice; Igf2p-, Igf2 paternal allele null mice; Igf1r-/-, Igf1r gene null mice; Igf2rm-, Igf2r maternal allele null mice. Deletion of Igf2r plus Igf2 results in a birth weight 60% of normal, similar to the size of mice with knockout of Igf2 alone, with no effect on neonatal survival. Indeed, specific deletion of Igf2 in the placenta causes small placenta and growth retardation. Deletion of Igf1r resulted in birth weights 45% of normal with 100% neonatal lethality. Studies have shown that this midsection is the site responsible for interaction with cell surfaces. It has a consensus nuclear translocation sequence, and translocation is facilitated by importin-B. It is present mostly as a nonglycosylated form of 24 kDa, with the glycosylated form being 29 kDa. It is widely expressed in embryonic tissues, fibroblasts, osteoblastic cells, prostatic cells, ovarian cells, and liver. It is 28 kDa and contains a glycosylation site in the highly variable midregion of the protein. The primacy of the role of estrogen comes from animal studies21 as well as reports of human subjects with mutations. A mutation of the estrogen receptor in a man was associated with tall stature and open epiphyses,22 and similar findings were reported in patients with mutations of the gene encoding the aromatase enzyme. Notably, dihydrotestosterone, a nonaromatizable androgen, can accelerate linear growth in boys. Thyroid hormone also has a direct effect on chondrocytes and osteoblasts, which both express thyroid hormone receptors. Thyroid hormone regulates chondrocyte proliferation and stimulates terminal differentiation, mineralization, and angiogenesis. The adolescent rise in serum gonadal steroid levels is an important part of the pubertal growth spurt. In addition, it is the stimulation of epiphyseal fusion by the pubertal rise of gonadal steroid production that results in the ultimate cessation of linear growth. Both androgens and estrogens increase skeletal maturation and accelerate growth plate senescence. Developmental or functional abnormalities of the hypothalamus account for most "idiopathic" cases of hypopituitarism, and recent molecular studies have begun to elucidate the molecular bases of these disorders. It is anticipated that most cases of idiopathic hypopituitarism will be defined at the genetic level in the future. Anencephaly results in a pituitary gland that is small or abnormally formed and is frequently ectopic. Despite the loss of hypothalamic regulation, somatotrophs differentiate and proliferate, although in diminished overall mass. Further indirect evidence in studies314 of isolated, complete anterior pituitary aplasia indicates that hypothalamic hypopituitarism and breech delivery are consequences of congenital midline brain defects, although perinatal residua of breech delivery may exacerbate ischemic damage to the hypothalamic-pituitary unit. Most of these children have hypothalamic dysfunction as the cause of diminished pituitary hormone secretion. In the older group, as in the infants, structural, acquired hypothalamic, stalk, or pituitary abnormalities must be considered.
Over time herbs native to outland buy geriforte 100 mg mastercard, patients are encouraged to pick up the pace as tolerated and to increase the duration and frequency of exercise sessions slowly to avoid overuse injuries herbals on york carlisle pa geriforte 100 mg generic. It is not unreasonable to suggest to patients that if they are going to incorporate exercise into their diabetes management program, they must think of exercise as a treatment that takes the place of a pill and requires adherence to produce benefit. All individuals should be encouraged to reduce sedentary time, particularly by breaking up extended amounts of time (>90 minutes) spent sitting. Also, it is essential to have patients critically assess the nature of any hypoglycemic symptoms that may occur. It is important to advise patients to vary the time of the day at which blood glucose levels are checked. For some patients, the highest blood glucose of the day is the morning glucose, whereas for others the highest is before bed. Particularly in early diabetes, gestational diabetes, and well-controlled diabetes, monitoring 1 to 2 hours after meals allows patients to assess the effect of their lifestyle and pharmacologic efforts in controlling postprandial glucose levels, which are usually the only glycemic abnormality present. Monitoring (and thus targeting therapy) at just one time of day can leave the patient with a less than ideal overall response to therapy. When glucose control is poor, having patients concentrate on premeal glucose levels is adequate. Once the premeal glucose levels reach the low 100s, many advocate that patients switch to checking 1- to 2-hour postprandial glucose levels; the latter approach amplifies the observed effect of diet on glycemic control and enables patients to see that moderate changes in meal plan, activity, and medications have a significant impact on glycemic control. Even after substantial inappropriate changes in food intake, activity, or timing or dose of medication, blood sugar values often return to near-normal levels overnight or by the time of the next meal. Many clinicians ask patients to monitor at least once a day (at varying times before a meal, at bedtime, and at midsleep) as well as with hypoglycemic symptoms. Unfortunately, such services usually are not reimbursed and can become an unsustainable burden on health care teams. One of the most difficult areas in which to keep current is the area of available equipment and supplies, particularly for glucose monitoring. A useful resource in this regard is the annual Consumer Guide, which is published as the January issue of Diabetes Forecast, a magazine for laypeople with diabetes and their families. The available oral antihyperglycemic agents can be divided by mechanism of action into several groups: insulin sensitizers with primary action in the liver, insulin sensitizers with primary action in peripheral tissues, insulin secretagogues, agents that slow the absorption of carbohydrates, insulins, agents that increase the activity of the incretin system, agents that increase glucose clearance into the urine, and novel agents whose influence on carbohydrate metabolism is still unclear. Although metformin has been available in Europe for over 40 years, it has been approved in the United States only since 1995. The major clinical activity of metformin is to reduce hepatic gluconeogenesis and glucose production. Because of its limited duration of action, it is usually taken at least twice daily, although a sustained-release formulation is available. Because biguanides do not increase insulin levels, they are not associated with a significant risk of hypoglycemia. The most common adverse events are gastrointestinal: nausea, diarrhea, crampy abdominal pain, and dysgeusia. About one third of patients have some gastrointestinal distress, particularly early in their course of treatment. This distress can be minimized by starting with a low dose once daily with meals and titrating upward slowly (over weeks) to effective doses. Sustained-release metformin is associated with less frequent and less severe upper gastrointestinal symptoms, the more common of the adverse effects of metformin, but it can increase the frequency of diarrhea, a much less common adverse effect overall. Most patients note no adverse effects with metformin therapy, and at least 90% tolerate it adequately with long-term use. Perhaps as a result of clinical or subclinical gastrointestinal effects, metformin is associated with less weight gain than other antihyperglycemic agents, and in some studies it has been associated with a modest weight loss. Some patients taking metformin develop progressive vitamin B12 deficiency; supplementation with relatively high doses of vitamin B12. The maximal daily dose of 2550 mg does not generally provide additional benefit beyond that seen at 2000 mg daily. Newer formulations of metformin combined with various classes of oral antihyperglycemic agents have been developed to maximize glucose-lowering effectiveness with a single prescription through the synergy of two classes of agents with different actions. Arguably, metformin has the best record among oral antihyperglycemic agents in outcome studies.
However herbs uses order geriforte 100mg fast delivery, the common combination of vascular disease with minor trauma can lead to ulceration herbalsmokeshopcom order 100mg geriforte free shipping. Minor injury and subsequent infection increase the demand for blood supply beyond the circulatory capacity, and ischemic ulceration and risk of amputation develop. Early identification of those patients who are at risk for peripheral vascular disease is essential, and appropriate investigation involving noninvasive studies, together with arteriography, often leads to bypass surgery to improve blood flow to the extremities. Distal bypass surgery is often performed, with good short-term but mixed long-term results in terms of limb salvage. The presence or absence of a dorsalis pedis or posterior tibial pulse is the simplest and most reliable indicator of significant ischemia that can be elicited at the bedside. Approximately 5% to 10% of diabetic patients have had past or present foot ulceration, and 1% have undergone amputation. A large community-based study in the United Kingdom showed an annual incidence of ulceration of approximately 2%; this rose to 7% with known diabetic neuropathy and to as high as 50% with a past history of ulceration. Even in experienced diabetic foot clinics, more than 50% of patients with new foot ulcers give a past ulcer history. OtherDiabeticComplications Patients with retinopathy and renal dysfunction are at increased risk for foot ulceration. A and B, Two lateral views of a patient with typical signs of a high-risk neuropathic foot. Notice the small-muscle wasting, clawing of the toes, and marked prominence of the metatarsal heads. At presentation with type 2 diabetes mellitus, this patient had severe neuropathy with foot ulceration on both the right foot (shown here) and the left foot. The combination of proprioceptive loss due to neuropathy and the prominence of metatarsal heads leads to increased pressures and loads under the diabetic foot. High pressures, together with dry skin, often result in the formation of callus under weight-bearing areas of the metatarsal heads. The presence of such plantar callus has been shown in cross-sectional and prospective studies to be a highly significant marker of foot ulcer risk. Conversely, removal of plantar callus is associated with a reduction in foot pressures and therefore a reduction in foot ulcer risk. In 1999, a North American/United Kingdom collaborative study1006 assessed the risk factors that resulted in ulceration in more than 150 consecutive foot ulcer cases. From this study, a number of causal pathways were identified, but the most common triad of component causes- neuropathy, deformity, and trauma-was present in 63% of incident ulcers. Prevention of Foot Ulceration and Amputation That diabetic foot ulceration is largely preventable is not disputed; small, mostly single-center studies have shown that relatively simple interventions can reduce amputations by up to 80%. Because foot ulcers precede most amputations, are among the most common causes of hospital admission for patients with diabetes, and account for much morbidity and even fatality, the widespread application of preventive foot care strategies is urgently required. Patients with any type of diabetes require regular review and screening of the feet for evidence of risk factors for foot ulceration, irrespective of disease duration. Of all the long-term complications of diabetes, foot problems and their risk factors are probably the easiest to detect. No expensive equipment is required, and the feet can be examined for evidence of neuropathic and vascular deficits in the office setting using simple equipment. A simple neurologic examination should include assessment of pressure perception using a 10-g monofilament; in a large U. A comparison of two diabetic foot ulcer classification systems: the Wagner and the University of Texas wound classification systems. Comprehensive foot examination and risk assessment: a report of the Task Force of the Foot Care Interest Group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. The orthotist, or shoe fitter, is invaluable to advise about and sometimes design footwear to protect high-risk feet, and these members of the team should work closely with the diabetologist and the vascular and orthopedic surgeons. Patients with risk factors for ulceration require preventive foot care education and frequent review.
Some of these metabolites are deconjugated in the intestine and reabsorbed into the enterohepatic circulation kisalaya herbals limited order 100 mg geriforte with mastercard. These coactivators link the receptor complex to the basal transcription apparatus yak herbals pvt ltd buy geriforte 100 mg without a prescription, thereby regulating transcription of target genes. Approximately 30% to 35% of this calcium is absorbed; however, losses from intestinal secretion of calcium lead to a net daily uptake of approximately 200 mg. Absorption of calcium and magnesium is impaired by bile salt deficiency, unabsorbed free fatty acids in steatorrheic states, and high dietary content of fiber or phytate. Gastric acid is needed to promote dissociation of calcium from anionic components of food or therapeutic preparations of calcium salts. Administration of calcium salts with meals, especially in achlorhydrics, and use of divided doses or more soluble salts such as calcium citrate are commonly employed strategies to increase calcium bioavailability. Calcium is thought to be absorbed by two pathways: a saturable transcellular pathway and a nonsaturable paracellular route. Although the necessity of vitamin D for paracellular calcium absorption remains controversial, substantial evidence exists that the hormone enhances this pathway as well. This pathway is thought to involve three steps: entry of calcium into the enterocyte (which is the rate-limiting step), transport across the cell, and extrusion across the basolateral membrane. The activity of these proteins correlates with active calcium transport; however, a causal relationship remains to be established. Arrows indicate that the hexamers found in the upregulated rat osteocalcin gene are variants of a consensus sequence, repeated here with identical orientations (direct repeats). The best studied effect of vitamin D on the enterocyte is the induction of synthesis of the intestinal calcium-binding protein, calbindin-9K. The affinity of calbindin for calcium is approximately four times that of the brush border calcium-binding components, so calcium is preferentially transferred to calbindin. Calbindin serves to buffer the intracellular free calcium concentration during calcium absorption. It associates with microtubules and may play a role in the transport of calcium across the enterocyte. Vitamin D administration has been shown to increase the concentration of troponin C, a calcium-binding protein in muscle that plays a role in excitation coupling and increases the rate of uptake of calcium by the sarcoplasmic reticulum. The myopathy that accompanies vitamin D deficiency is characterized by normal creatine phosphokinase levels, a myopathic electromyogram, and biopsy findings of loss of myofibrils, fatty infiltration, and interstitial fibrosis. The myopathy resolves within days to weeks of vitamin D replacement and does not correlate with normalization of mineral ion homeostasis. Several analogues have been shown to have antiproliferative effects on normal cells as well as on malignant cells in vitro and in xenografts in immunosuppressed mice. This suggests that such analogues may be useful in the prevention and treatment of hyperparathyroidism. The antiproliferative effects of vitamin D have been exploited clinically in the treatment of psoriasis. The physiology underlying the differential biologic effects of these analogues is not completely understood. In contrast, the concentrations of these mineral ions in extracellular fluid are quite comparable. Extracellular calcium and phosphate, in particular, exist so close to the limits of their mutual solubility that stringent regulation of their concentrations is required to avoid diffuse precipitation of calcium phosphate crystals in tissues. Serum concentrations and total body balances of the mineral ions are maintained within narrow limits by powerful, interactive homeostatic mechanisms. In contrast, the mechanisms of the phosphate sensing needed for normal homeostasis are not understood. Dietary calcium restriction, for example, is followed by an increase in the efficiency of intestinal calcium absorption. Enhanced intestinal calcium absorption is quantitatively the most important response to calcium deprivation, but a series of other homeostatic events also occur that limit the impact of this stress. Major homeostatic responses to dietary calcium deprivation or loading are depicted. Arrow thickness indicates relative activity of transport or secretory mechanisms, whereas amounts of hormones or transported ions are related to the size of their notations. Note that the extracellular calcium concentration is well maintained, although different underlying mechanisms are involved in the two circumstances (see text for details).
Syndromes
- Caffeine
- Did you notice a fullness or lump in the abdomen?
- Peripheral artery disease
- Ultrasound of the heart (echocardiogram)
- Febrile convulsions
- Redness around the anus
- Barbituates
In addition herbals and surgery discount geriforte online amex, about twice as many subjects randomized to orlistat lost at least 5% or at least 10% of their initial body weight wicked x herbal cheap 100mg geriforte mastercard, compared with those randomized to placebo. Approximately 70% to 80% of subjects treated with orlistat experienced one or more gastrointestinal events, compared with 50% to 60% of those treated with placebo. Subjects rarely reported more than two episodes despite continued orlistat treatment. Orlistat treatment can also affect fat-soluble vitamin status and the absorption of some lipophilic medications. These two agents were combined in an effort to get synergistic weight loss while using lower doses than usually required for each drug alone, in an effort to reduce the adverse side effects of each medication when given at their normal full dose. If less than 3% weight loss after 12 weeks does not occur with the recommended dose, it is advised to discontinue or advance to top dose by providing the transition dose for 2 weeks. If less than 5% weight loss is achieved after 12 weeks on the full dose, treatment should be stopped by taking the medication every other day for 1 week and then discontinue completely. In an intention-to-treat analysis after 1 year of therapy, the placebo-subtracted weight loss was approximately 9% for the top dose and approximately 6. In addition, cognitive impairment (attention or memory deficits) can occur, and there is a potential risk of fetal toxicity in pregnant women treated with topiramate (topiramate monotherapy exposure during pregnancy is associated with twofold to fivefold increased prevalence of oral clefts). The data from most studies on the effect of metformin on body weight indicated that metformin does not cause weight gain and that treatment with metformin reduces the amount of weight that is gained with other diabetes medications. The recommended dose is 10 mg twice a day; if a patient has not lost at least 5% of baseline body weight by 12 weeks, it is recommended to discontinue drug treatment. The most frequent adverse effects of lorcaserin in these studies were headache, dry mouth, dizziness, and nausea. There was no difference in the development of cardiac valvulopathy between drugtreated and placebo-treated subjects at 1 or 2 years. Additional eligibility criteria are the inability to maintain weight loss with conventional therapy, acceptable operative risks, absence of active substance abuse, and ability to comply with the long-term treatment and follow-up required. Typically, six adjustments are made in the first year after band placement, as needed to enhance weight loss. Bowel continuity is restored via an anastomosis between the Roux limb and the excluded biliopancreatic limb approximately 75 to 150 cm distal to the gastrojejunostomy. Sleeve gastrectomy involves dividing the stomach along its vertical length, removing approximately 75% of the stomach, and creating a banana-shaped sleeve. Biliopancreatic diversion involves a horizontal gastrectomy, leaving behind 200 to 500 mL of stomach, which is anastomosed to the small intestine, 250 cm from the ileocecal valve. The excluded biliopancreatic limb is anastomosed to the ileum, 50 cm from the ileocecal valve. The distal 50-cm common channel is where digestive secretions from the biliopancreatic limb mix with the ingested food delivered by the alimentary limb. Biliopancreatic diversion with duodenal switch involves constructing a 150- to 200-mL vertical sleeve gastrectomy with preservation of the pylorus and formation of a duodenal-ileal anastomosis. The excluded biliopancreatic limb is anastomosed to the ileum, 100 cm from the ileocecal valve, where digestive secretions and nutrients mix. Both biliopancreatic diversion and biliopancreatic diversion with duodenal switch cause considerable malabsorption. Several observations from clinical studies have led to the concept that bypassing the upper gastrointestinal tract has additional benefits on glucose homeostasis beyond weight loss alone. The overall early and late mortality rate is about 0% to 2%; the risk of complications and death is influenced by the type of procedure, experience of the surgeon, presence of a competent bariatric surgery team and hospital, and medical status of the patient. Approximately three fourths of the deaths that occur are caused by anastomotic leaks and peritonitis, and one fourth are caused by pulmonary embolism. Most complications that occur with any gastrointestinal surgical procedure also occur after bariatric surgery, including atelectasis, pneumonia, deep vein thrombosis, pulmonary embolism, anastomotic leak with peritonitis, wound infection, gastrointestinal bleeding, and internal hernias. In addition, not all patients lose a lot of weight, and some patients who lose weight initially regain most or all of their lost weight over time. No uniform definition of diabetes remission has been used routinely in bariatric surgery studies. Remission has most often been defined as the withdrawal of all diabetes medications, in conjunction with a normal fasting plasma glucose concentration (ranging from <100 to <126 mg/dL), or a normal HbA1c (ranging from <6% to <7%).
The tumor arises from rests of squamous cells at the junction of the adenohypophysis and neurohypophysis and forms a cyst as it enlarges; the cyst contains degenerated cells and may calcify but does not undergo malignant degeneration herbal salvation purchase geriforte 100mg. The cyst fluid ranges from the consistency of machine oil to a shimmering herbals guide generic 100mg geriforte with visa, cholesterol-laden liquid, and the calcifications may be microscopic or gross. About 75% of craniopharyngiomas arise in the suprasellar region; the remainder resemble pituitary adenomas. Mutations in -catenin have been found in patients with adamantinomatous craniopharyngiomas. The most common presentation results from increased intracranial pressure and includes headaches, vomiting, and oculomotor abnormalities. Visual field defects result from compression of the optic chiasm, and papilledema or optic atrophy may be present. Visual and olfactory hallucinations have been reported, as have seizures and dementia. Most children with craniopharyngiomas have evidence of growth failure at the time of presentation, and they are often found retrospectively to have had reduced growth since infancy. Operative intervention via craniotomy or transsphenoidal resection may result in partial or almost complete removal of the lesion. Postoperative irradiation is commonly used, especially if tumor resection was incomplete. Patients with a history of hypothalamic obesity associated with craniopharyngiomas undergoing brain surgery were favored to have sustained weight loss. Pituitary adenomas (see Chapter 9) are infrequent during childhood and adolescence, accounting for fewer than 5% of patients undergoing surgery at large centers. There is a variable experience as to the invasive nature of pituitary adenomas, but the prevailing opinion is that they are less aggressive in children than in adults. The patients with macroadenoma had an approximately 50% incidence of hypopituitarism, compared with zero incidence in those patients with microadenomas; long-term cure rates were between 55% and 65% for both tumor sizes. The localized or generalized proliferation of mononuclear macrophages (histiocytes) characterizes Langerhans cell histiocytosis, a diverse disorder that occurs in patients of all ages, with a peak incidence at ages 1 to 4 years. The degree of pituitary stalk thickness has been shown to correlate with long-term risk outcomes. In the latter group, an evolving neurodegenerative syndrome (identified in 10% of patients with 15-year follow-up) seemed to be associated with pituitary involvement. Members of a well-described pedigree from Ecuador were from an inbred population with Mediterranean origins. Even in those disorders in which the pathology is not primarily within the endocrine system, there is often an underlying hormonal abnormality contributing to the growth failure. Marasmus refers to an overall deficiency of calories including protein malnutrition. Kwashiorkor refers specifically to inadequate protein intake, although it may also be characterized by some caloric undernutrition. Decreased weight growth usually precedes the failure of linear growth by a very short time in the neonatal period and by several years at older ages. Stunting of growth due to caloric or protein malnutrition in early life often has lifelong consequences, including diminished skeletal growth. Some of these conditions may be further characterized by deficiencies of specific dietary components, such as zinc, iron, and vitamins necessary for normal growth and development. Anorexia nervosa and bulimia are extremes of "voluntary" caloric deprivation that are commonly associated with impaired growth before epiphyseal fusion, which may result in diminished final adult height. Notice that crossing of percentiles on the weight curve preceded that on the height curve, and that, after caloric intake was normalized (arrow), gain in weight occurred before improvement in linear growth. Intestinal disorders that impair absorption of calories or protein cause growth failure, for many of the same reasons as malnutrition per se. Celiac disease (gluten-induced enteropathy) and regional enteritis (Crohn disease) should be considered in the differential diagnosis of unexplained growth failure. Documentation of malabsorption requires demonstration of fecal wasting of calories, especially fecal fat, along with other measures of gut dysfunction such as the D-xylose or breath hydrogen studies. The prevalence of celiac disease in children being evaluated for short stature is approximately 5%. After 8 years of growth impairment, the patient was placed on a gluten-free diet and demonstrated substantial catch-up growth, returning to the previous growth percentiles.
Glomerulonephritis treated with alternate-day glucocorticoid therapy leads to a late herbals supplements discount 100 mg geriforte amex, diminished equine herbals geriforte 100mg on line, but prolonged pubertal growth spurt that can result in a normal final height. Children with early onset of leukemia and long-term remission experience puberty at an appropriate age or with only a slight delay, whereas patients with initial symptoms of leukemia in late childhood may have considerable delay of pubertal development. Long-term follow-up studies demonstrate the rising incidence of the metabolic syndrome survivors and high lifetime risk for cardiovascular disease in childhood cancer. Poorly controlled diabetes mellitus can lead to poor growth, fatty infiltration of the liver, and sexual infantilism. Prepubertal children are most vulnerable to poor glycemic control, and pubertal subjects exhibit normal growth unless severe hyperglycemia occurs. Cushing disease can be associated with delayed onset or arrest of gonadarche, although excessive virilization is an alternative finding. Anorexia nervosa,543 a common cause of gonadotropin deficiency in adolescence, is a functional disorder. Prevalence is increased among girls (it is the third most common chronic disease of adolescent girls), and it starts at ever-younger ages, but it is rare in boys. This condition has the highest mortality rate of all psychiatric disorders544; weighted mortality rates. Significantly low weight is defined as a weight that is less than minimally normal or, for children and adolescents, less than that minimally expected. Intense fear of gaining weight or of becoming fat, or persistent behavior that interferes with weight gain, even though at a significantly low weight. Subtype: Restricting type Binge-eating/purging type the onset of amenorrhea precedes the onset of severe weight loss. The pathogenesis is multifactorial and includes a genetic factor and a well-characterized psychological component. Before the diagnosis of anorexia nervosa is made, organic disease must be excluded; for example a girl with macroprolactinoma may present with signs consistent with anorexia nervosa. The prevalence of anorexia nervosa is increased among individuals with Turner syndrome. Serum leptin levels are low, consistent with the strikingly decreased mass of adipose tissue, and increase with regain of weight. This condition must be considered in the differential diagnosis of growth failure in younger subjects. Lower heart rates are characteristic and a dangerous sign of severe disease and not to be confused with an athletic bradycardia in view of the excessive exercise the patient engages in. A lower systolic blood pressure, lower body temperature, anemia, and leukopenia are found in persons with anorexia nervosa. The ratio of bone age to chronologic age is significantly lower in girls with anorexia nervosa and correlates positively with duration of illness and markers of nutritional status. Treatment of decreased bone density in these individuals is accomplished with improved nutrition, and a degree of catch-up in bone density occurs, although reversion to normal may not occur. Normal endocrine and metabolic function may follow weight gain, but amenorrhea may persist for months, suggesting persistent hypothalamic dysfunction. In view of the associated mortality rate, parenteral alimentation may be indicated in resistant patients with severe weight loss, especially in those with infection or an electrolyte imbalance. However, refeeding syndrome with attendant hypophosphatemia may result if not handled appropriately. Treatment of this disorder requires skillful management, understanding, patience, and psychiatric consultation in a team approach. Unfortunately, evidence-based approach to optimal treatment is not plentiful, and the difficulty in obtaining therapy in uninsured individuals remains. The consequences range from severe estrogen deficiency to anovulation to a short luteal phase. Recurrent inappropriate compensatory behaviors in order to prevent weight gain, such as self-induced vomiting; misuse of laxatives, diuretics, or other medications; fasting; or excessive exercise. A history of childhood sexual abuse is more common than in unaffected adolescents. Cessation of growth can occur in infants and young children with psychosocial dwarfism. Stressful social situations can also inhibit growth and physical pubertal development at adolescence.
Typical and atypical associated findings in a group of 346 patients with Mayer-Rokitansky-KuesterHauser syndrome herbs books geriforte 100mg otc. Persistent unexplained congenital clitoromegaly in females born extremely prematurely zenith herbals purchase geriforte on line. Predictors of posttraumatic stress in parents of children diagnosed with a disorder of sex development. Adult women with 21-hydroxylase deficient congenital adrenal hyperplasia, surgical and psychological aspects. Timing of surgery for feminizing genitoplasty in patients suffering from congenital adrenal hyperplasia. Health status of adults with congenital adrenal hyperplasia: a cohort study of 203 patients. Relationship between final height and health outcomes in adults with congenital adrenal hyperplasia. Increased cardiovascular and metabolic morbidity in patients with 21-hydroxylase deficiency: a Swedish population-based national cohort study. Suboptimal psychosocial outcomes in patients with congenital adrenal hyperplasia; epidemiological studies in a nonbiased national cohort in Sweden. A phase 2 study of Chronocort, a modified-release formulation of hydrocortisone, in the treatment of adults with congenital adrenal hyperplasia. Psychosexual development in adolescents and adults with disorders of sex development-results 963 485. Male patients with partial androgen insensitivity syndrome: a longitudinal follow-up of growth, reproductive hormones and the development of gynaecomastia. Whether linear growth occurs as a continuous process or with periodic bursts of growth and arrest1-4 has been hard to characterize definitively. There do appear to be seasonal variations of growth, with slower growth in autumn and winter and greater growth in spring and early summer. Deviation from such a normal pattern of growth can be the first manifestation of a wide variety of disease processes, including endocrine and nonendocrine disorders and involving virtually any organ system of the body. Therefore, frequent and accurate assessment of growth is of primary importance in the care of children. Laboratory and radiologic investigations include an evaluation for occult systemic disease and exclusion of hormonal abnormalities. Measurement Assessment of growth requires accurate and reproducible determinations of height. Supine length is routinely measured in children younger than 2 years of age, and erect height is assessed in older children. It can be useful to measure both length and height in children between 2 and 3 years of age to allow comparisons with prior length measurements and to begin to record height measurement for ongoing comparisons. The inherent inaccuracies involved in measuring length in infants are often obscured by the rapid skeletal growth during this period. Optimally, the child should be relaxed, the legs should be fully extended, and the head should be positioned in the Frankfurt plane, with the line connecting the outer canthus of the eyes and the external auditory meatus perpendicular to the long axis of the trunk. When children are old enough (and physically capable) to stand erect, it is best to employ a wall-mounted Harpenden stadiometer similar to that designed by Tanner and Whitehouse for the British Harpenden Growth Study. The traditional measuring device of a flexible arm mounted to a weight balance is notoriously unreliable and does not provide accurate serial measurements. But growth and final height can also be affected by external factors, including the quality and quantity of nutrition, and by psychosocial factors. This process is regulated by multiple hormones and growth factors interacting with an array of membrane receptors that activate seemingly redundant intracellular signaling cascades. Height determinations should be performed by a trained individual rather than an inexperienced member of the staff. We recommend that lengths and heights be measured in triplicate, that variation should be no more than 0. For determination of height velocity when several measurements are being made within a short period, the same individual should perform the determinations to eliminate interobserver variability. Even when every effort is made to obtain accurate height measurements, a minimum interval of 6 months is necessary for meaningful height velocity computation.