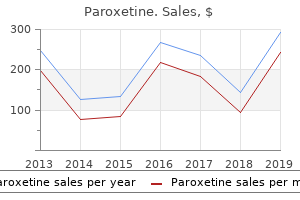
"Buy paroxetine australia, medications similar to abilify".
By: K. Jaroll, M.S., Ph.D.
Co-Director, Stony Brook University School of Medicine
Cheap 20mg paroxetine fast delivery
Additionally symptoms xanax treats 10mg paroxetine sale, tumors medicine 7 day box 10 mg paroxetine visa, thyroiditis, and infiltrative disease can be uncommon causes of goiters. The formation and growth of numerous nodules in the thyroid gland cause the characteristic massive enlargement of the neck. Beatrice Diaz: Application Suspecting thyroid dysfunction, the endocrinologist orders thyroid function tests. On the basis of clinical and laboratory findings, the endocrinologist diagnoses Ms. The plan is to reevaluate her status in approximately 6 weeks and decide on radioactive iodine131 ablation therapy or thyroidectomy to permanently treat her Graves disease. Approximately 2 weeks later, she notes a recurrence of diaphoresis, palpitations, tremors, hyperreflexia, heat intolerance, and feelings of anxiety and nervousness. She also notes dyspnea on exertion and weakness of the muscles in her shoulders and thighs. She is admitted to the hospital for observation to evaluate for possible cardiac arrhythmias. Her thyroid function tests are monitored for 2 years, after which time she is lost to follow-up. Thyroid Nodules the term thyroid nodule refers to an abnormal growth of thyroid cells that forms a lump within the thyroid gland. These nodules are often asymptomatic and detected by the patient but may be revealed during physical examination or a radiologic procedure such as carotid ultrasonography. The discovery of a thyroid nodule necessitates a diagnostic workup, particularly to exclude cancer. Multinodular goiter, Hashimoto thyroiditis, and follicular adenomas (benign tumors) are the primary causes of benign thyroid nodules. An autonomous hyperfunctioning nodule that secretes excessive amounts of T3 and T4 is associated with hyperthyroidism and related clinical signs and symptoms. Obstructive symptoms, cervical lymphadenopathy, vocal cord paralysis, and the presence of a hard fixed mass are suggestive of a malignancy. Clinical manifestations of goiters are associated with the type of thyroidal dysfunction. One of the risks of long-standing goiters is obstruction due to progressive compression of the trachea or a sudden increase in size from a nodular hemorrhage. A thyroid scintigraphy (thyroid scan) is a nuclear medicine procedure that visually identifies the functional status (hyperfunctioning or hypofunctioning) of thyroid tissue on the basis of the selective uptake of various radionuclides. The tissue is examined by a cytopathologist and classified as benign, nondiagnostic or unsatisfactory, malignancy or suspicious for malignancy, or atypical or follicular neoplasm. Although rare, the infection can be caused by a variety of organisms and may occur in immunocompromised or debilitated individuals and older adults. Acute infectious thyroiditis is associated with sudden onset of neck pain, thyroid tenderness, fever, chills, dysphagia, and neck swelling. The diagnosis can be made through fine-needle aspiration and culture; the infection is then treated with appropriate antibiotics. Linking Pathophysiology to Diagnosis and Treatment Although the biochemical manifestations of thyroiditis vary according to etiology, most thyroid disorders share the feature of inflammation. Some patients may experience pain and tenderness of the thyroid and surrounding structures; some may be asymptomatic. Thyroiditis Thyroiditis encompasses a group of disorders characterized by inflammation of the thyroid gland that can result in hyperthyroidism, hypothyroidism, or a nontoxic euthyroid goiter. Primary Hyperthyroidism Hyperthyroidism, also referred to as thyrotoxicosis, is the synthesis and release of excessive quantities of thyroid hormone. The most common causes of primary hyperthyroidism are Graves disease and toxic multinodular goiter. Etiology, Pathogenesis, and Clinical Manifestations Hashimoto thyroiditis, a form of autoimmune thyroid disease, is discussed later in the chapter.
Buy paroxetine australia
Rollins demonstrates clinical manifestations of a patient with advanced ovarian cancer symptoms you need glasses cheap paroxetine master card, including nausea and vomiting symptoms 7 days post iui order paroxetine 20mg with amex. From the initial workup, she was diagnosed with a bowel obstruction secondary to cancer. Rollins and her family to discuss the progression of her disease and to develop an appropriate and acceptable plan of care. A venting gastrostomy consists of a tube placed through the skin into the stomach to allow air and liquid to escape into a drain. The tube can be used both for decompression and as a means of providing nutrition when the obstruction resolves. Rollins on the day after her admission to the hospital, but it is unsuccessful because the tumor burden in her abdominal cavity prevents the team from being able to visualize the stomach wall. Rollins, who is admitted to the program after being discharged to home following a 4-day hospitalization. Cachexia is skeletal muscle wasting and involuntary weight loss resulting from both metabolic abnormalities and a lack of nutrition. Nutritional deficiencies ultimately produce ketosis, leading to a lack of interest in food. Depression, anxiety, and delirium are among the many comorbidities that can contribute to anorexia and cachexia. These metabolic changes lead to weight loss, adipose tissue loss, and skeletal muscle wasting. Asthenia, a loss or lack of physical strength, is a consequence of skeletal muscle wasting. In patients with cancer and other inflammatory conditions, the immune system produces chemical mediators that lead to these changes. Specific mediators, called proinflammatory cytokines, include tumor necrosis factor, interleukin-1, interleukin-6, and interferon. These mediators also may contribute to anorexia by acting on the hypothalamus to decrease hunger sensation. Unlike starvation, in which there is depletion of adipose tissue to spare skeletal muscle protein, in cachexia both adipose tissue and skeletal muscle are depleted. In cachexia, there is a shift from normal daily synthesis of skeletal muscle proteins to muscle protein degradation to provide substrates for enhanced hepatic synthesis of acute-phase proteins involved in the inflammatory response. A thorough physical examination may reveal loose skin turgor, dry mouth and thirst, confusion and drowsiness, difficulty clearing pulmonary secretions, abdominal discomfort, and decreased urine output. Subjectively, along with stating a decreased or lack of appetite, patients may complain of fatigue, diminished overall body strength, and pain with eating. Thompson has had an unintentional weight loss of 40 pounds that occurred over the 3 months before he was admitted to hospice. This weight loss and his anorexia, which is a contributing factor, and the resultant fatigue cause much distress for both Mr. What strategy could the nurse use to help the family cope with this visible change in Mr. The diagnosis of cachexia is based on the clinical manifestations described in the previous section. Every effort is made to make appealing foods and fluids available to palliative care patients (see the Impact of Nutrition in Clinical Practice feature). The healthcare team is sensitive to the concerns of family members who may feel that they are failing or abandoning the patient by not feeding him. It is helpful to inform them that decreased intake of foods and fluids can lead to ketosis and subsequent release of endorphins that contribute to an enhanced sense of well-being and diminished discomfort. Disease-related problems include oral or systemic infections, poorly fitting dentures, pain or difficulty swallowing associated with eating, physical obstruction to dietary intake, and impaired absorption of dietary nutrients. For example, in end-stage chronic obstructive pulmonary disease, the increased work of breathing may leave few energy reserves for the effort required to eat and digest food. Chronic high levels of inflammatory cytokines shift metabolism toward increased degradation of protein and fat and increased production of glucose to provide substrates for synthesis of acute phase proteins, which are involved in the inflammatory response. Anorexia and cachexia both contribute to involuntary weight loss, loss of adipose tissue, and skeletal muscle wasting. Corticosteroids such as dexamethasone and prednisone may help to increase appetite and physical strength for a short time.
| Comparative prices of Paroxetine |
| # | Retailer | Average price |
| 1 | Sherwin-Williams | 623 |
| 2 | Brinker International | 348 |
| 3 | Wendy's / Arby's Restaurants | 851 |
| 4 | RadioShack | 679 |
| 5 | Lowe's | 505 |
| 6 | Bed Bath & Beyond | 490 |
| 7 | BJ'S Wholesale Club | 939 |
Paroxetine 10 mg generic
The capillaries of the liver lobule are called sinusoids and are located between the hepatocytes medicine education buy paroxetine 10 mg with amex. The role of the sinusoids is to receive blood from both the hepatic artery and the portal vein and to remove foreign materials from the blood treatment quotes purchase paroxetine 20 mg line. When asked where the pain in located, he points to the left upper quadrant of his abdomen and moves his finger around his rib cage to his back and shoulder. Sudden, intense left upper abdominal pain that radiates to the back and sometimes the shoulder suggests inflammation of what organ The superior mesenteric vein brings blood to the liver from the small intestine and the ascending and transverse sections of the large intestine as well as the stomach. The inferior mesenteric vein collects blood from the descending region of the large intestine and the rectum to contribute to the hepatic portal system. The inferior mesenteric vein and the splenic vein connect with the larger superior mesenteric vein to form the hepatic portal vein. In the liver, the central veins join to become the hepatic veins, moving blood out of the liver to the inferior vena cava and back to the heart. The liver requires a higher volume of blood supply to accomplish numerous functions in the body, including storage, excretion, metabolism, digestion, glucose regulation, detoxification, and hematology. Vascular functions include storage of blood for use as needed by the body during hemorrhage or hypovolemia. Fat-soluble vitamins (A, D, E, and K), vitamin B12, the minerals iron and copper, and glucose and fat are stored in the liver and used to maintain homeostasis. Glycogen storage in the liver helps the body regulate the blood sugar with the conversion of glycogen to glucose. The rich blood supply via the portal vein brings drugs, bacteria, pathogens, toxins, and other foreign substances from the gastrointestinal system to the liver, where filtration takes place. Metabolism of carbohydrate, protein, and fat occurs in the liver, along with the production of proteins involved in coagulation. Albumin and globulin are other major proteins that the liver is responsible for producing. Albumin maintains the osmotic pressure; globulins are used for cellular enzymatic reactions. Bilirubin is a brownish-yellow substance that is produced when the liver breaks down red blood cells. Bile leaves the liver in the common hepatic duct and goes to the cystic duct of the gallbladder. Food entering the small intestine stimulates the hormone secretin in the duodenum to produce bile. Bile breaks fat into small globules, thus making more surface area available for chemical digestion to finish the digestive process. Excretion of bilirubin and cholesterol is completed with bile transport to the feces, where the substances are eliminated from the body. The liver breaks down and detoxifies many substances, including medications, steroid hormones, and alcohol. Liver function tests are often ordered as a panel to help get an overall laboratory analysis of the liver function. Albumin, which is produced in the liver, is essential for maintenance of the oncotic pressure, thus helping to maintain the vascular system. Ammonia is a by-product of protein metabolism that is converted to urea in the liver. With liver dysfunction, the liver is not able to convert ammonia to urea; as a result, toxic levels of ammonia accumulate in the blood, causing systemic damage. This form of bilirubin is lipid soluble and must be transformed to a water-soluble product to be excreted. Albumin carries unconjugated bilirubin to the liver, where it detaches from the albumin and is then conjugated to a water-soluble product. Removal of this conjugated bilirubin is accomplished with bile salts that enter the intestine from the common bile duct. Albumin Albumin, a component of proteins, makes up more than half of plasma proteins. It increases osmotic pressure (oncotic pressure), which is necessary for maintaining the vascular fluid.
Discount paroxetine express
These surgical data in the management of pediatric refractory constipation that is unresponsive to both medical management and cecostomy highlight that these children should be evaluated with caution in an individualized manner medications ordered po are paroxetine 20mg with mastercard. As described earlier 3 medications that affect urinary elimination purchase on line paroxetine, the primary aim of medical treatment for constipationassociated fecal incontinence is to empty the impacted rectum and to maintain soft stools during follow-up. Sometimes antidiarrheal drugs, such as loperamide, are prescribed for children with fecal incontinence to reduce the fecal output. It further inhibits peristaltic movements and increases internal anal sphincter tone. In contrast to adults, experience with loperamide in childhood fecal incontinence is limited. One long-term follow-up study described that after 2 years of intensive medical and behavioral treatment only 29% of the children were successfully treated. Keeping records of completed toilet training and bowel movements in a diary can enhance motivation. Only 29% of children were having less than one episode of fecal incontinence in 2 weeks after 2 years of medical and behavioral therapy. However, this indicates that 15% of children progress to adulthood with fecal incontinence. Most children treated for constipation are eventually cured, although the time required for treatment varies and relapses are not uncommon. Therefore, it is important to provide support and encouragement through regularly scheduled office visits. Progress should be assessed and, if necessary, dosage adjustments need to be made. After regular bowel habits are established, the medication dosage is gradually decreased. A systematic review found that only half of all children with constipation followed for 6 to 12 months after therapy were doing well without laxatives. It is important to emphasize that constipation is a clinical diagnosis based primarily on symptoms in the absence of red flag symptoms, and therefore in the majority of patients no further testing is needed. The treatment consists of education, keeping a bowel diary, and toilet training four times a day following meals and immediately after coming home from school. Functional nonretentive fecal incontinence in children: a frustrating and long-lasting clinical entity. Constipationassociated and nonretentive fecal incontinence in children and adolescents: an epidemiological survey in Sri Lanka. Increased prevalence of constipation in pre-school children is attributable to under-consumption of plant foods: a community-based study. Children and adolescents with chronic constipation: how many seek healthcare and what determines it Review of organic causes of fecal incontinence in children: evaluation and treatment. An epidemiologic study of voiding and bowel habits in Korean children: a nationwide multicenter study. Constipation in children: novel insight into epidemiology, pathophysiology and management. Are anxiety and depression related to gastrointestinal symptoms in the general population Quality of life and somatic symptoms in children with constipation: a school-based study. Association of constipation and fecal incontinence with attention-deficit/hyperactivity disorder. Review article: fecal incontinence in children: epidemiology, pathophysiology, clinical evaluation and management. New insight into rectal function in pediatric defecation disorders: disturbed rectal compliance is an essential mechanism in pediatric constipation. Chronic childhood constipation is associated with impaired quality of life: a casecontrolled study.
Quality paroxetine 20mg
Eosinophilic esophagitis: Updated consensus recommendations for children and adults treatment 1st line order paroxetine with mastercard. Efficacy of dietary interventions for inducing histologic remission in patients with eosinophilic esophagitis: A systematic review and meta-analysis medications while breastfeeding buy paroxetine mastercard. Use and yield of endoscopy in patients with uncomplicated gastroesophageal reflux disorder. Trends and outcomes of hospitalizations for peptic ulcer disease in the United States, 1993 to 2006. Pathology of non-Helicobacter pylori gastritis: Extending the histopathologic horizons. Utility of magnetic resonance imaging for suspected appendicitis in pregnant women. Evaluation and management of small-bowel obstruction: An Eastern Association for the Surgery of Trauma practice management guideline. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. The liver is also responsible for numerous other functions in the body, including synthesis of plasma proteins, metabolism and elimination of drugs and toxins, and storage of vitamins, glucose, and blood. The exocrine pancreas aids in the digestion of carbohydrates, fats, and proteins with the production of enzymes as well as bicarbonate, which is needed to neutralize chyme in the duodenum. Each of these three accessory organs contributes a distinct aspect of the digestive process; all work together to get their secretions to the duodenum to assist in digestion. Case Studies the following cases will be addressed throughout the chapter to assist in applying chapter content to clinical situations that involve individuals with disorders of the exocrine pancreatic and hepatobiliary systems. His chief complaint is pain to his right upper quadrant of the abdomen that has been getting progressively worse for 2 weeks. He has experienced some weight loss and has not been eating much at meals, often feeling bloated and nauseated. The primary healthcare provider completes the assessment, noting mild jaundice, abdominal tenderness, and distention. The healthcare provider also orders the following laboratory tests: liver function tests, complete blood count, international normalization ratio, alkaline phosphatase, and alpha fetoprotein. What organs and structures are found in that area of the body that may contribute to his symptoms For patients with unexplained weight loss, evaluation should include diagnostic testing to rule out what condition Concepts Related to the Exocrine Pancreatic and Hepatobiliary Systems the liver is a metabolically complex and vascular organ that has a direct impact on all other organs and tissues in the body. As a result, the liver has the ability to interrelate many concepts, such as immunity, infection, metabolism, hemostasis, elimination, comfort, nutrition, energy balance, environment, and inflammation and oxidative stress. The pancreas and gallbladder play an important role in the digestive process and in nutrition, comfort, and metabolism. These concepts will be discussed as they relate to the pathogenesis of the exocrine pancreatic and hepatobiliary systems. Helen Martin: Introduction Helen Martin is a middle-aged female who is experiencing perimenopause. She and her husband Gil live in a blended household that includes several family members, a situation that contributes to her stress and anxiety. She is seen by her primary healthcare provider for complaints of digestive disturbances and abdominal pain after meals, especially fatty meals. This yellowing of the skin and sclera of the eyes is caused by what substance and suggests initial thoughts of pathology in which organ(s) What elements of the history suggest possible gallbladder disease in this patient Because the abdominal muscles of infants are weak, the abdomen normally tends to protrude. The hepatocytes produce enzymes that catalyze the various chemical reactions, making the liver capable of a variety of specific functions. A decrease in serum albumin will cause fluid to shift from within the vessels to the tissues, resulting in edema. Once the acute phase is over, the serum level will decrease promptly, whereas the serum bilirubin will remain increased. Ammonia Ammonia, a by-product of protein metabolism, is formed from bacterial action in the intestine and from metabolizing tissues.
Syndromes
- Excessive fear (paranoia)
- Recurrent or unnoticed injury to the hand or arm due to diminished sensation
- Reduced alertness (consciousness)
- Let your doctor know if you have ever had a reaction to contrast. You may need to take medicines before the test in order to safely receive this substance.
- Medicines to treat an infection, if present
- During treatment to see if the cancer is responding to treatment
- Fainting or near-fainting
- Endoscopy -- camera down the throat to see burns in the esophagus and the stomach
Discount paroxetine 20 mg visa
Large prospective pediatric studies are needed to assess the efficacy of commonly used and novel treatment modalities medications just like thorazine order cheap paroxetine. The treatment should be tailored to the child and family needs symptoms knee sprain cheap paroxetine uk, possibilities, and beliefs. The history taking should investigate the possible contributing factors for the individual patient and adapt the treatment to each situation. The Rome criteria is currently under revision to enhance research efforts and clinical care through better categorization of patients according to age and symptoms into separate disorders that may differ in pathophysiology and responsiveness to treatment. Children aged 10 to 17 years had the longest duration of abdominal pain (median 9. The author found that 53% of individuals with a history of recurrent abdominal pain had persistent gastrointestinal symptoms and that the index group had a higher prevalence of gastrointestinal symptoms compared to the control group. Children with persistent abdominal pain have been shown to have more anxiety, depression, and lower selfesteem, and more negative life events. This vulnerability persists into late adolescence and early adulthood regardless of the resolution of abdominal pain. The combination of not addressing cognitions on functional disorders and maladapted coping strategies in a timely fashion can lead to illnessrelated behaviors such as experiencing a disproportionate degree of disability and frequent health care consultation for nonspecific symptoms. An irritable bowel syndrome subtype defined by species-specific alterations in faecal microbiota. Multicenter, randomized, placebo-controlled trial of amitriptyline in children with func- 73 tional gastrointestinal disorders. Which of the following findings suggests an organic cause for chronic abdominal pain History and physical examination findings may suggest an organic cause in a patient presenting with chronic abdominal pain. Deceleration of linear growth, recurrent vomiting, chronic diarrhea (particularly at night), perianal disease, dysphagia, oral lesions, skin rashes, unintended loss of more than 10% of body weight, visible blood in stool or positive stool occult blood test, fever of unknown origin, delayed puberty and amenorrhea are among factors that suggest an organic cause. Studies have shown a significant benefit in using hypnotherapy and guided imagery for children with chronic abdominal pain. Behavioral and cognitivebehavioral psychological interventions are also treatments found to be effective in reducing nonheadache pain intensity and disability in children and adolescents. Gestalt therapy, psychoanalysis, depthpsychological techniques and Reiki have not been shown to provide a similar durable response. Gestalt therapy Psychoanalysis Depth-psychological techniques Reiki Hypnotherapy 73. A prospective schoolbased study of abdominal pain and other common somatic complaints in children. Parental report of abdominal pain and abdominal pain-related functional gastrointestinal disorders from a community survey. Overt and relational victimization among children with frequent abdominal pain: links to social skills, academic functioning, and health service use. Pain symptoms and stooling patterns do not drive diagnostic costs for children with functional abdominal pain and irritable bowel syndrome in primary or tertiary care. Functional abdominal pain in childhood and adolescence increases risk for chronic pain in adulthood. Adult outcomes of pediatric recurrent abdominal pain: do they just grow out of it Recurrent abdominal pain in children: forerunner to adult irritable bowel syndrome Recollection of childhood abdominal pain in adults with functional gastrointestinal disorders. The biopsychosocial approach to chronic pain: scientific advances and future directions. Stress-induced physiologic changes as a basis for the biopsychosocial model of chronic musculoskeletal pain: a new theory Irritable bowel syndrome in twins: heredity and social learning both contribute to etiology. Irritable bowel syndrome aggregates strongly in families: a family-based casecontrol study. Cytokine gene polymorphisms are associated with irritable bowel syndrome: a systematic review and meta-analysis.
Generic paroxetine 20 mg with mastercard
In this situation symptoms 3 dpo buy paroxetine 10 mg on-line, the local agency for child protective services should be called medicine for anxiety buy generic paroxetine from india. Diagnosis and treatment of these feeding disorders requires a multidisciplinary team that may include nutrition, occupational therapy, hearing and speech, psychology, and psychiatry, in addition to medical subspecialists. Children with this disorder are at increased risk for future developmental difficulties. Home visiting by trained lay visitors may be helpful for some of these infants,30 although an initial inpatient admission is necessary in severe cases or when the safety of the child is in question. The child may be distractible while feeding, even during the first few months of life, although this condition often develops somewhat later at the time of transition to spoon-feeding or self-feeding. It is characterized by the acute onset of severe and consistent refusal of solids, liquids, or all textures. Children with this disorder show distress in anticipation of feeding and may refuse to swallow food placed in the mouth. Preterm infants and those with suck-swallow incoordination may be at particular risk for a posttraumatic feeding disorder. However, hospital admission may be warranted if neglect is suspected, when a patient is at risk for refeeding syndrome, or when outpatient management fails. The pressuring or coaxing tactics that parents may use to encourage their children to eat can be counterproductive, and are associated with increased food refusal even in the absence of sensory food aversion. This situation may occur when families are overly concerned about obesity and cardiovascular disease,33 or are fearful about food allergies or gluten sensitivity. On the other hand, nonspecific abnormalities may also lead to unnecessary anxiety and further workup. For instance, a finding of low serum bicarbonate may lead to further testing for renal tubular acidosis, leading to frequent "overcalls" of acidosis and potentially unwarranted subspecialist referrals. Zinc deficiency may itself contribute to poor growth, by causing anorexia, immune dysfunction, and poor deposition of muscle. Zinc supplementation trials have had an overall positive effect on both weight and height. However, supplementation of these particular micronutrients has not proven to improve growth in the absence of anemia or severe vitamin A deficiency. Diarrhea may become more apparent to parents after weaning or after introduction of solid foods to the diet. Among infants, the presence of gross blood in the stool or positive stool guaiac testing is frequently indicative of milk protein intolerance and should prompt consideration of a dairy-free diet. At any age, a decrease in stool pH or the presence of reducing substances is suggestive of carbohydrate malabsorption, although may also indicate other gastrointestinal conditions such as small intestine bacterial overgrowth. A marked elevation in spot fecal fat is suggestive of pancreatic insufficiency, such as in cystic fibrosis versus intestinal malabsorption, and may warrant testing of fecal elastase. Generally, neutral fat in the stool is more consistent with pancreatic insufficiency, whereas split fat is more consistent with intestinal fat malabsorption. The presence of a large number of small drops of split fat in the stool frequently indicates concomitant lactose maldigestion associated with mucosal injury. Malnutrition can itself cause small bowel atrophy and villous blunting, and in addition can directly suppress lactase expression by enterocytes. In those cases, it is generally preferable to use a ready-to-feed nutrient-dense formula if it is available. Otherwise, one can use an "energy supplemented" formula such as a powdered infant formula mixed to high concentration or with added fats or carbohydrates. Energy supplemented formulas may have inappropriate solute load or inadequate nutrient density, and are prone to contamination and errors in mixing. In a study comparing the use of nutrient-dense to energy-supplemented formulas in infants with poor growth, caloric intake and weight gain were the same, but the nutrient-dense formula group received 42% more protein and 15% to 40% more vitamins and minerals, and maintained a normal mean blood urea concentration.
Discount 10mg paroxetine with visa
If the hypoglossal or glossopharyngeal nerves are injured symptoms gallbladder problems buy paroxetine 10 mg free shipping, the movement of the tongue is compromised medications ritalin buy paroxetine 10mg online, and the tongue often falls back into the oral pharynx and obstructs the larynx. Other causes of airway obstruction in trauma patients include (in order of frequency) blood, loose teeth, vomitus, and foreign objects. Multiple facial fractures, especially Le Fort type fractures (facial fractures that cause a separation of the facial bones), could cause either a complete or partial airway obstruction. To clear the airway, a jaw-thrust maneuver is recommended because this has been proven to cause the least manipulation to the cervical spine. This is known as the head-tilt/chin-lift maneuver and must be done very carefully, as it could worsen any spinal injury. Any compromise to the airway must be immediately cleared, and if the patient cannot protect his or her own airway, then airway control must be obtained. If the patient answers in a clear, normal voice, the healthcare provider can assume that the airway is patent. However, any sign of vocal difficulties suggests a compromise to the vocal cords and may be a sign of airway compromise. A nasal airway is best used for patients who are conscious; an oral airway is recommended for unconscious patients because it is very uncomfortable and often stimulates a gag response in conscious patients. If airway and breathing are both compromised, then immediate intubation and ventilatory support are required. When a fracture to the bone is such that the layers of the bone are separated and the bone is in danger of becoming disrupted or separating, an unstable fracture exists. An in-line fracture, or stable fracture, is one that occurs within the bone structure and the bone remains strong and intact. Cervical vertebrae 3, 4, and 5 house the nerves in the spinal column that are responsible for normal respiration. If this area of the spinal cord is compromised, the patient will not be able to breathe. Therefore, cervical spine stability must be maintained constantly while the airway is inspected. For that reason, "A" represents airway and cervical spine immobilization as the highest priority in trauma care. Therefore, there is a natural passive flexion of the cervical spinal column in infants. To prevent further flexion to the cervical spine, the healthcare provider must be cautious not to hyperextend the neck when opening the pediatric airway. A supraglottic airway, such as a laryngeal mask airway, may also provide support until a more definitive airway can be established in patients without complete obstruction. Rapid sequence intubation consists of administering high-flow oxygen via a nonrebreather mask or bag-valve-mask. After the patient is pre-oxygenated, a sedative is administered intravenously followed by a paralytic agent. If this technique is not successful, then manual ventilations must be immediately resumed. If the patient cannot be ventilated while paralyzed, a surgical airway must be rapidly obtained. However, Spinal Cord Injury Spinal cord injuries are among the most devastating injuries in trauma patients. The vast majority of these deaths are attributed to high-level spinal cord injuries. As cells in the spinal cord begin to die, further damage to the spinal cord results, causing secondary injury to the spinal cord and extending the degree of damage in an ascending pattern. For this reason, patients with spinal cord injury must be closely monitored for further ascending deterioration of the spinal cord. Because C3, C4, and C5 are involved in respiration, monitoring the peak airway flow of the patient will be a good indicator as to the progression of respiratory weakness, indicating the progression of the spinal injury. A review of the anatomy and physiology of the spinal column is important to understand this very complicated injury. Immediately after a spinal cord injury, a series of physical, chemical, and biochemical changes occur that result in an array of clinical manifestations. Once the spinal cord has been injured, there is an uncoupling of oxidative phosphorylation and a shift to anaerobic glycolysis.
Order 20mg paroxetine
The severity of myocardial injury varies widely from a minor area of bruising on the myocardium to severe medicine that makes you poop discount paroxetine 20mg without prescription, massive damage resulting in necrosis and myocardial stunning symptoms cervical cancer generic paroxetine 20mg free shipping. If the myocardium is stunned, it will not contract efficiently enough to maintain a cardiac output that can sustain life, and this relatively small group of patients will not survive a severe myocardial contusion. Tachycardia is the most common sign of cardiac contusion and is present in approximately 70% of patients diagnosed with a cardiac contusion. Cardiac enzymes are also not specific for 1262 Chapter 51 the Pathophysiology of Primary and Secondary Traumatic Injury cardiac contusions; however, there is some evidence that an increased level of cardiac troponin indicates myocardial injury. A young, healthy trauma patient suffering a mild myocardial contusion will usually survive with no cardiac sequelae. This has proven to be the time when dysrhythmias are most likely to occur, and virtually no life-threatening injuries have been reported more than 12 hours after injury. However, if any signs of myocardial compromise exist, the patient must be admitted to a monitored bed. Finally, in the most severe cases, when the myocardium is stunned or bruised to the point of pump failure or cardiac cellular necrosis, treatment includes myocardial rescue, hyperperfusion to drive the cardiac output, and inotropic pharmacologic support. The injury is associated with a pneumothorax or hemothorax in 3% of cases and then is nearly always associated with multiple ipsilateral rib fractures. Clavicular fractures that are not associated with ligamentous or vessel injury often can be treated with a sling or figure eight brace. Falls, blast injuries, and highvelocity missile wounds can also cause a pulmonary contusion. Signs and symptoms of a pulmonary contusion range from shortness of breath, cough, and mild tachypnea to hypoxia, hypoxemia, and respiratory arrest. Chest x-ray will demonstrate patchy, irregular infiltrates over the area of injury. Treatment of a pulmonary contusion is directly related to the severity of the injury. In mild cases of pulmonary contusion in a young, healthy, stable patient, the patient can simply be observed for any signs of compromise. More aggressive treatment of pulmonary contusion consists of pulmonary support, aggressive pulmonary toileting, and pain management. Respiratory support can include supplemental oxygen by face mask, a continuous positive airway pressure or bilevel positive airway pressure device, or mechanical ventilation. However, careful fluid resuscitation is important, as overhydration can cause further injury. Some of these aggressive therapies include high-pressure ventilation, hypercapneic ventilation, prone positioning, use of high-frequency oscillating ventilation, and extracorporeal membrane oxygenation. Abdominal Injury the word abdomen is derived from a Latin word meaning "to hide," and that is exactly what occurs with abdominal trauma: the injury is hidden in the abdomen. For this reason, patients who suffer injuries to the abdomen present a difficult diagnostic challenge to healthcare providers. It is imperative to consider underlying structures in determining the specific injuries resulting from abdominal trauma. The most frequently injured abdominal organ is the spleen (46%), followed by the liver (33%). Penetrating abdominal injuries typically result from stab wounds, gunshot wounds, or lacerations.
Order paroxetine from india
Inflammatory bowel disease and adenomas in mice expressing a dominant negative N-cadherin treatment brown recluse bite cheap paroxetine 10 mg without a prescription. Desquamative enteropathy and pyloric atresia without skin disease caused by a novel intracellular 4 integrin mutation treatment 2014 buy generic paroxetine line. Impact of intestinal permeability, inflammation status and parasitic infections on infant growth faltering in rural Bangladesh. Intestinal inflammation measured by fecal neopterin in Gambian children with enteropathy: association with growth failure, Giardia lamblia, and intestinal permeability. Chronic T cell-mediated enteropathy in rural West African children: Relationship with nutritional status and small bowel function. Chemokines and chemokine receptors in mucosal homeostasis at the intestinal epithelial barrier in inflammatory bowel disease. Human duodenal epithelial cells constitutively express molecular components of antigen presentation but not costimulatory molecules. Induction of protective IgA by intestinal dendritic cells carrying commensal bacteria. Rapid transepithelial antigen transport in rat jejunum: impact of sensitization and the hypersensitivity reaction. A dominant, coordinated T regulatory cell-IgA response to the intestinal microbiota. A bacterial carbohydrate links innate and adaptive responses through Toll-like receptor 2. The requirement of intestinal bacterial flora for the development of an IgE production system fully susceptible to oral tolerance induction. Segmented filamentous bacteria are potent stimuli of a physiologically normal state of the murine gut mucosal immune system. Treg induction by a rationally selected mixture of Clostridia strains from the human microbiota. Tolerogenic dendritic cells induced by vitamin D receptor ligands enhance regulatory T cells inhibiting autoimmune diabetes. High and low vitamin A therapies induce distinct FoxP3+ T-cell subsets and effectively control intestinal inflammation. Vitamin A deficiency inhibits intestinal adaptation by modulating apoptosis, proliferation, and enterocyte migration. Comparative anatomy and phylogenetic distribution of the mammalian cecal appendix. Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. Mucus enhances gut homeostasis and oral tolerance by delivering immunoregulatory signals. Bacterial translocation in the normal human appendix parallels the development of the local immune system. Surfactant proteins in the digestive tract, mesentery, and other organs: evolutionary significance. Contributions of dendritic cells and macrophages to intestinal homeostasis and immune defense. Uptake through glycoprotein 2 of FimH(+) bacteria by M cells initiates mucosal immune response. The multifaceted influence of the mucosal microflora on mucosal dendritic cell responses. Human intestinal epithelial cells promote the differentiation of tolerogenic dendritic cells. Deficiency of indoleamine 2,3-dioxygenase enhances commensal-induced antibody responses and protects against Citrobacter rodentium-induced colitis. A distinct array of proinflammatory cytokines is expressed in human colon epithelial cells in response to bacterial invasion. Role of mast cells in intestinal mucosal function: studies in models of hypersensitivity and stress.
References: